Alzheimer’s disease (dementia) NCLEX review for nursing students!
This review will discuss a type of dementia known as Alzheimer’s disease. It’s vital a nurse knows how to provide care with this type of disease.
You will learn the following information in this review:
- What is Alzheimer’s disease?
- Pathophysiology
- Nurse’s Role
- Testing
- Medications
Don’t forget to access the free Alzheimer’s disease quiz when you’re done reviewing this material.
What is Alzheimer’s Disease?
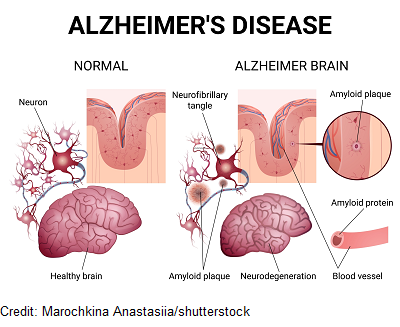
It’s a chronic brain disease that is a type of dementia. It occurs because neurons in the brain lose the ability to communicate and eventually die. This is mainly due to the development of plaques and tangles.
These plaques and tangles lead to a progressive loss of the ability to:
problem solve, communicate, recall memories, perform everyday tasks, and care for one self.
Eventually, as the disease progresses, the person will be completely dependent on someone for care. It is not reversible and no cure is currently available. Medications are available to help manage symptoms.
Interesting Facts about Alzheimer’s Disease
According to the CDC.gov:
- 5th leading cause of death among adults 65 or older
- 6.2 million Americans had Alzheimer ’s disease in 2021
- Cases of this disease are expected to increase to 14 million by 2060
- Women are more likely to develop this disease than men (because they tend to live longer).
- Hispanics and African Americans are at a higher risk.
- Signs and symptoms tend to appear after the age of 60 (but it could happen earlier).
- Risk Factors: family history, age, gender, diabetes, heart disease, smoking
- This is a disease that becomes progressively worst and can be organized into stages. Some patients progress slowly through the stages, while others may go fast through them.
- The exact cause of Alzheimer’s disease is not fully understood but plaques and tangles seem to be the common problem.
Therefore, as you can see from the facts above this is a chronic disease that gradually becomes worse until the patient is unable to function. It is very debilitating for the patient and creates a major impact for family members (who tend to be the caregivers) and healthcare workers. If family can’t provide care to the patient, care will be provided in a skilled nursing facility.
As a nurse you will definitely be caring for patients with this disease. So to help us understand how to provide care to a person with Alzheimer’s disease, let’s talk about the pathophysiology.
Pathophysiology of Alzheimer’s Disease
This disease affects the brain, specifically neurons that make up certain areas of the brain. First let’s review the neuron:
Neuron:
We have billions of neurons in our brain that are always talking to each other and sending messages. This is how we are able to function. To communicate, they send electrical signals and release neurotransmitters at their synapse, which sends a unique message to other nerve cells, muscles, or glands.
The message sent depends on the type of neurotransmitter released. There are many different types of neurotransmitters in the body. As a side note, there are two neurotransmitters I want you to remember: acetylcholine and glutamate. These neurotransmitters are targeted with medications used to treat this disease.

The structure of the neuron is made up of a cell body. This contains the nucleus which gives it structure and helps keep things running smoothly for the neuron.
The dendrites, which remind me of tree branches waiting from something to land on them, receive information for other nerves cells and take that message to the cell body. The axon takes information it receives away from the cell body and to other dendrites of neurons or another structure.
Now, around the neuron are cells that help protect its ability to function. One type of cell is called the microglia. It provides safety to the neuron by keeping it safe from damage by removing dangerous material.
So, in order for the neuron to work, it must be intact and free from anything that can impede communication like tangles or plaques. In Alzheimer’s disease, neurons lose the ability to communicate, thrive, and then die.
Why do they do this?
Development of Plaques and Tangles:
First, let’s talk about plaques:
Beta-amyloid plaques are found in between neurons (outside them).
These plaques are made up of beta-amyloid proteins that form between neurons and result in impediment of communication. How do they get there?
Let’s look at the cell membrane of the nerve cell:
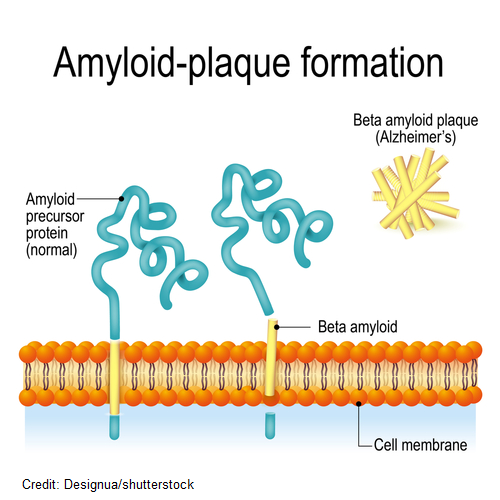
Crossing through the cell membrane is a protein called APP (amyloid precursor protein). As it crosses over through the membrane, enzymes from outside and inside the cell membrane cause this protein to breakdown into small pieces of peptides.
Normally, these peptides that have broken off from the APP will be metabolized and removed from outside the neuron. However, in Alzheimer’s disease the enzyme that is helping the beta amyloid peptide break off isn’t working right. Therefore, large strands of beta-amyloid peptides are created. These peptides are not metabolized correctly and start to congregate between neurons creating plaques.
This will cause problems with neuron communication and inflammation occurs, which damages the neuron and it eventually dies. These plaques collect in various parts of the brain and lead to the decline in brain functioning.
Now, outside the neuron (as I pointed out in the neuron section) there are cells that help protect the neuron. One type is called the microglia and its job is to keep the environment of the neuron nice and tidy (so it eats any debris hanging out). When it sees these plaques it causes a major inflammatory response, which makes things worst for the neuron.
Neurofibrillary tangles are found inside the neuron.
These tangles are made up of a protein called Tau. This protein plays a role in providing structural strength to the microtubules in the neuron.
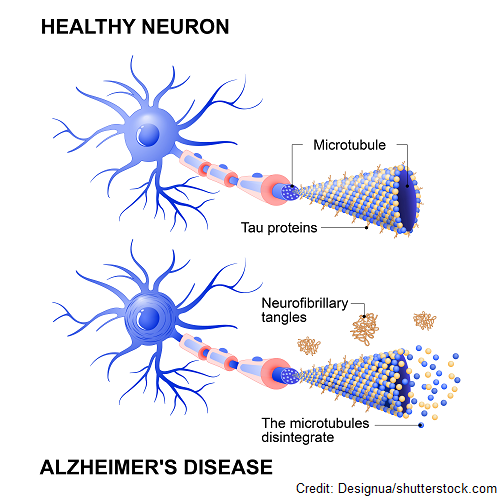
Microtubules play a vital role in helping deliver nutrients throughout the neuron and helps give it shape. However, in Alzheimer’s disease Tau proteins quit working and begin to change. This causes the microtubules to fall apart (which is going to affect how nutrients are delivered within the neuron).
Unfortunately, the Tau proteins start to clump together. This forms neurofibrillary tangles. These tangles will affect how the neuron works inside and will eventually lead it to die. When neurons quit communicating and die, this leads the brain tissue to become smaller called brain atrophy.
NOTE: there is some controversy regarding the tangle theory, so our scientific understanding of Alzheimer’s disease may change as additional research is performed.
Now let’s review the parts of the brain because this will help us understand the signs and symptoms found in a patient with Alzheimer’s disease.
The Brain
Our brain can be divided into different sections based on their function. These functions of each part of the brain can help us understand why certain signs and symptoms appear with this disease.
During the early parts of this disease, brain changes start to occur before signs and symptoms actually appear.
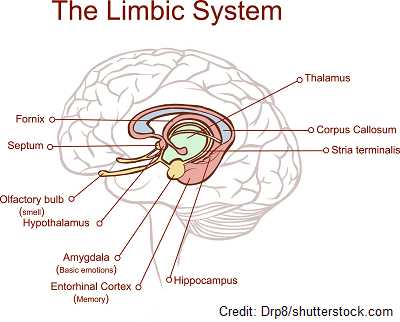
Alzheimer’s disease tends to start and affect the structures deep in the central part of the brain. For example, the hippocampus is affected early on. This area of the brain is responsible for learning and memory (forming new memories like fact-based memories and spatial memory which helps you navigate around).
Close by this structure and also affected is the entorhinal cortex, which plays a role with understanding time, direction, and memory. In addition, the amygdala, which plays a role with emotional memory, is affected. Therefore, as you can see these structures share the role of some type of memory. This is why usually the first sign of Alzheimer’s disease is related to memory loss.
Later on in the disease, the cerebral cortex is affected. The cerebral cortex is the outside layer in the brain that surrounds the top of the cerebrum. Therefore, we’re talking about a huge part of the brain.
The cerebral cortex is made up of different lobes (frontal, parietal, temporal, and occipital lobes) that are responsible for different brain functions like our emotions, ability to process thoughts and solve problems, plan, reason, and communicate language. In Alzheimer’s disease these lobes can be affected, which leads to corresponding symptoms in the patient.

Now let’s start talking about the signs and symptoms of this disease. There are some important terms used to describe some signs and symptoms seen in a patient with this disease. You want to know these for exams and in practice.
The helpful thing about these terms, since we are talking about Alzheimer’s disease (which starts with the letter A), is that all these terms start with the letter A and end with ia:
Apraxia: inability to perform a certain motor activities (ex: can’t perform the movements to use a toothbrush or fork)
Aphasia: can’t understand speech or create speech to communicate
Agnosia: can’t recognize everyday objects, people, or interpret their senses (taste, sound, smell etc.)
- Ex: can’t recognize people (forget their spouse or children) or a place, bowel and urine incontinence (don’t understand the sensation to use the bathroom)
Amnesia: memory loss (starts with short and them progresses to long term)
- can’t remember the year or current date (time), can’t tell you what they did that day (early on until the disease spreads they can remember childhood memories but not about a recent memory but as the disease spreads long-term memories will be gone), repeats themselves because they forgot they told you, forgets about important events
Anomia: inability to recall the name of objects…may make up words to call the object
Stages of Alzheimer’s Disease
These signs and symptoms develop over time and progressively get worst. The progression of Alzheimer’s disease can be organized into the following stages:
Preclinical Alzheimer’s Disease:
- Changes occurring in the brain but no symptoms noted….can happen over years.
Mild Cognitive Impairment
- Memory changes that are subtle but doesn’t affect their activities.
- Forgetting things especially recent commitments, new people they’ve met, or conversations, start to get confused on places or time, feels like something isn’t right…can’t think clearly
- Can last for several years
Mild Alzheimer’s (Early-stage):
- Typically when the Alzheimer’s Disease is diagnosed
- Mild forgetfulness that is noticed by others, and it’s starting to affect some parts of their functioning…short-term memory problems (losing objects frequently or can’t remember new material just learned), repeating self or asking the same questions, language problems start (can’t think of the word), mental instability like depression, confusion, insomnia
- Still can function and be independent but during this time patient needs to be planning for the future (end of life care and plans, estate planning etc.)
- Last a couple of years
Moderate Alzheimer’s Disease (Middle Stage):
- Confusion now sets in that affects how the patient can function and they will need help (safety is an issue along with self-care)
- judgement is lapsed: safety an issue, getting lost, wandering, forgetting how to cook or use objects like with hygiene, needs help with bathroom, how to dress depending on the weather, confusing family members, insomnia, mental instability: episodes of anger and anxiety, hallucinations
- Sundowner’s Syndrome: as the day gets closer to evening the patient’s confusion increases with intense periods of agitation and hallucinations
- Patient able to move around and engage in activities (that are simple) but must be monitored.
- Intense time for caregivers because patient must be monitored at all times and requires a lot of care
- Longest stage
Severe Alzheimer’s Disease: (Late Stage)
- Severe symptoms
- Language communication minimal along with motor activities, spends much time in bed or sitting needs
- Problems swallowing and eating
- due to this they are at risk for lung infections like pneumonia
- Needs constant care
- Interacting with the patient still very important, use nonverbal and touch as needed, have calming music on during the day
Testing for Alzheimer’s Decease
As pointed out earlier, the brain in undergoing changes before the patient actually has symptoms. Early detection is key in helping the patient prepare and get treatment (that doesn’t cure) but helps symptoms.
In order for a physician to diagnose this disease they must do investigative work because there is NOT one conclusive test for Alzheimer’s disease at this time. Many different tests are used because other conditions can present as this disease like a brain injury, stroke, or tumor.
Tests can include:
Cognitive assessments (tests thinking, memory, and judgement), mental evaluations, diagnostic imaging, biomarker tests, genetic testing
Diagnostic Imaging: looks at brain changes and rules out any other causes….example: MRI, CT and/or amyloid PET scan (looks for beta amyloid in the brain)
Biomarkers tests: assesses cerebrospinal fluid (CSF) through a spinal tap for beta-amyloid and tau proteins, and recent new blood test that can assess for biomarkers in the blood
Genetic testing: used for research not routinely ordered….Apolipoprotein E (ApoE-4)…a positive result doesn’t necessarily mean a person will develop the disease.
Nursing Interventions & Treatment for Alzheimer’s Disease
Role: Identifying signs and symptoms of the disease, educating patient and caregivers, helping patient through the stages (understanding how it progresses, what to expect, medications, testing, end of life care), helping caregivers (immense responsibility for caregiver…identify stress, respite care help, navigating through the disease)
The middle and severe stage of this disease is when the patient is going to start needing the most help and care. The 7 M’s can help guide us through our role as the nurse.
7 M’s
Memory: often reorient patient, remind patient and show how to use objects they have forgotten how to use (display signs on objects as reminders), keep tasks simple (they have problems with complicated instructions…causes agitation), don’t belittle the patient for forgetting
Movement (help keep the patient as independent as the disease allows because this helps with motor skills and body strength): maintain routines, incorporate exercises, easy fun games and things that are easy they like to do
Mental Health: keep calm during outbursts and use calm voice, provide with distractions and give time to respond, don’t hurry patient, be aware of Sundowner’s in some patients and prepare (encourage a calm relaxing environment)
Sundowner’s Syndrome triggers:
- exhaustion (needs period of rest)
- sickness
- low lighting (not enough time in the sunlight)
- medications
- caffeine (limit at night)
Hallucinations of the senses: see, feel, taste and hearing things…keep calm and be understanding to the patient, acknowledge feelings, remove things that may make the hallucinations worse: outside noises, keep areas well-lit to prevent shadows and remove reflective objects
Maintain Safety: poor judgement (no driving, cooking alone or using dangerous objects), as the disease progress tasks need to be very simple and safe
Watch for wandering (patient loses the ability to recognize places and people along with keeping time) can become lost very easily
- watch for signs they are starting to get lost or forget places, taking longer than normal to return from a place or having trouble finding rooms in the house, or talking about going somewhere they use to go all the time or visit someone
- early evening is when many patients began to get confused more and wander
- triggers: unfamiliar, crowded places, needing a basic need met like drink/food, use the bathroom, trying to do a routine they have always done before the disease
Interventions for Wandering:
WANDER
Wear a medical identification bracelet or GPS tracking device (disguised as a watch or placed in the shoe)
Avoid stressful, unfamiliar places (crowds, loud areas this can confuse and stress the patient which causes wander)
Needs met: bathroom, food, and liquid needs
Display signs that provide cues to the patient: label the rooms of the house on their doors and place reminders or warning signs
Exercise important: needs an organized day that has periods of activities they enjoy (create a safe place for the patient to wander and walk) and rest
Remove assess to doors or windows by keeping them locked with alarms and obscure the locks and alarms, hide keys to car
Maximize communication: as disease progresses patient will start to have more problems with communicating and the nurse will have to tailor how to communicate with patient based on their ability…even in the late stage communication is very important to provide a loving and caring environment
Communication Interventions
PATIENT
Pick one question or instruction step to give at a time (repeating may be necessary)
Avoid correcting or arguing (intense tones or anger facial expression can cause stress)
Take time for patient to speak and respond
Identify yourself directly in front of patient rather than behind (patient may react in a fearful or impulsive way)
Eye contact on eye level rather than standing is important (feels less intimidating to the patient)
Nonverbal communication helpful especially in late stage: act out, point, or use images
Talk in a normal tone that is clear and slow (not loud and fast), eliminate outside noises
Medical Needs
Hygiene: regular bathing, grooming, and mouth care,incontinence…needs ample times to use the bathroom, skin care, help with selecting outfits that are easy to put on limit buckles, buttons and weather appropriate (as the disease progresses the patient loses the ability to make judgement calls about hygiene and dressing)
Hydration: loses sense of thirst or can’t effectively tell you they’re thirsty, needs easy access to refreshment (measure how much taking in) and offer variety of hydration (popsicles, smoothies etc.)
Nourishment: forgets to eat, loses interest, trouble swallowing “dysphagia” this can occur as the disease progresses and leads to pneumonia: speech language pathologist to evaluate: may need thickened liquids and soften food consistency
Interventions for Encouraging the Patient to Eat:
don’t overwhelmed with options (serve one food item at a time), healthy options that they patient likes to eat (healthy fats, proteins, vegetables, and fruits, limit sugars, and salts), finger foods that are soft and easy to chew/swallow (issues with use utensils), help patient focus on meal…short attention span so keep environment well-lit, encourage family members to eat with the patient
Medications
Needs help with organizing medications and how to take them, may forget to take, or overdose
Meds don’t cure but can help management symptoms of Alzheimer ’s disease:
Cholinesterase Inhibitors
Remember “DR. G”: Donepezil, Rivastigmine, Galantamine
Cholinesterase inhibitors inhibit the enzyme, cholinesterase, from breaking down the neurotransmitter acetylcholine.
Acetylcholine is a neurotransmitter that has many functions with one of them being memory and thinking abilities. Therefore, by preventing the breakdown of this neurotransmitter, more acetylcholine is available for use in the brain.
Patients with this disease may have low levels of acetylcholine because nerve cells like the cholinergic neurons that work with this neurotransmitter don’t work.
Side effects: GI upset (nausea, vomiting, and diarrhea)….give with food, muscle spasms, bradycardia (risk for falls…monitor heart rate)
N-methyl D-aspartate antagonist (NMDA antagonist)
Memantine: this medication is for moderate to severe dementia, may be taken with cholinesterase inhibitors
It affects the neurotransmitter glutamate. This is a neurotransmitter that likes to excite neurons. It does this by working with NMDA receptors to cause calcium to enter the cell that fires up the neuron. This is a normal process that helps us learn and maintain our mood. BUT if that is happening in excess with too much glutamate being made (like what may be happening in Alzheimer’s disease) it can lead to neuron damage and it dies.
NMDA antagonists limit how glutamate can engage the NMDA receptor so too much calcium can’t fire up the neuron and lead to damage.
Side effects: headache, dizzy (falls), constipation (monitor bowel movements)
Aducanumab ***no longer prescribed starting in 2024…now lecanemab or donanemab is used : new medication given IV infusion about every 4 weeks…. for early stages of Alzheimer’s disease
Decreases beta-amyloid plaques which can help increase cognitive function…needs diagnostic testing to confirm plaques present like spinal tap or amyloid PET scan
Side effects: brain swelling or bleeding (will need MRIs to monitor the brain for Amyloid-Related Imaging Abnormalities (ARIA)
References:
Centers for Disease Control and Prevention. (2021, June 22). Alzheimer’s disease. Centers for Disease Control and Prevention. Retrieved June 7, 2022, from https://www.cdc.gov/dotw/alzheimers/index.htm
Center for Drug Evaluation and Research. (2021, June 7). FDA’s decision to approve new treatment for alzheimer’s disease. U.S. Food and Drug Administration. Retrieved June 8, 2022, from https://www.fda.gov/drugs/news-events-human-drugs/fdas-decision-approve-new-treatment-alzheimers-disease
How is alzheimer’s disease treated? National Institute on Aging. (2021, July 8). Retrieved June 8, 2022, from https://www.nia.nih.gov/health/how-alzheimers-disease-treated
Stages of alzheimer’s. Alzheimer’s Disease and Dementia. (n.d.). Retrieved June 7, 2022, from https://www.alz.org/alzheimers-dementia/stages
Tips to make mealtimes easier for people with alzheimer’s. National Institute on Aging. (n.d.). Retrieved June 8, 2022, from https://www.nia.nih.gov/health/infographics/tips-make-mealtimes-easier-people-alzheimers
The truth about aging and dementia. Centers for Disease Control and Prevention. (2019, August 20). The Retrieved June 7, 2022, from https://www.cdc.gov/aging/publications/features/Alz-Greater-Risk.html
U.S. Department of Health and Human Services. (2022, February 17). Blood test can predict presence of beta-amyloid in the brain, new study finds. National Institute on Aging. Retrieved June 8, 2022, from https://www.nia.nih.gov/news/blood-test-can-predict-presence-beta-amyloid-brain-new-study-finds