Potassium-sparing diuretics NCLEX pharmacology review for nursing students!
Potassium-sparing diuretics are medications that help remove extra fluid volume from the blood through increased urination. This review will discuss the mechanism of action of potassium-sparing diuretics, what conditions they treat, nursing implications, side effects, and patient education.
Don’t forget to take the potassium-sparing diuretics quiz after reviewing this material.
Potassium-Sparing Diuretics Lecture
Potassium-Sparing Diuretics Pharmacology NCLEX Review
Always ask yourself these 5 questions when you see a drug name to help you understand how the drug works, your role as a nurse, and what information will be asked on an exam about the drug:
Name (specifically the family name)? This will tell how the drug works.
Used for? This will tell you WHY the drug was ordered…what condition is this medication treating in your patient?
Responsibilities as the nurse? This will tell you what your role is as the nurse and what you need to monitor in the patient.
Side effects? Know the common side effects of the medications
Education pieces for the patient? As the nurse we play a HUGE role in educating our patients on how to take the drug, what to watch out for, and when to call the doctor.
Now, using those 5 questions let’s go over what you need to know about potassium-sparing diuretics for exam:
Name?
- Potassium-sparing diuretics: these medications don’t cause HYPOkalemia (like the other diuretics we’ve discussed, such a loop diuretics and thiazide diuretics)
- They work on the distal parts of the nephron, specifically the last part of the distal tubule and collecting duct. This is where they alter the sodium and potassium exchange within the nephron.
- This leads to less sodium being reabsorbed back into the bloodstream, which leads to a diuretic effect (remember water loves sodium and will stay with it) causing the patient to have increased urination.
How they work?
Since potassium-sparing diuretics are indeed diuretics, they affect how the nephrons of the kidneys work.
What is a nephron? Each kidney has millions of nephrons that function to filter the blood and “tweak” that filtered material created by the glomerulus. When I’m referring to “tweaking” the filtrate, this means that the substances in the filtrate will either be reabsorbed back into the bloodstream, excreted out of the body as urine, or the body will secrete substances it doesn’t need into the filtrate. This process is based on what the body needs, and different sections of the nephron has its own job for how it “tweaks” the filtrate.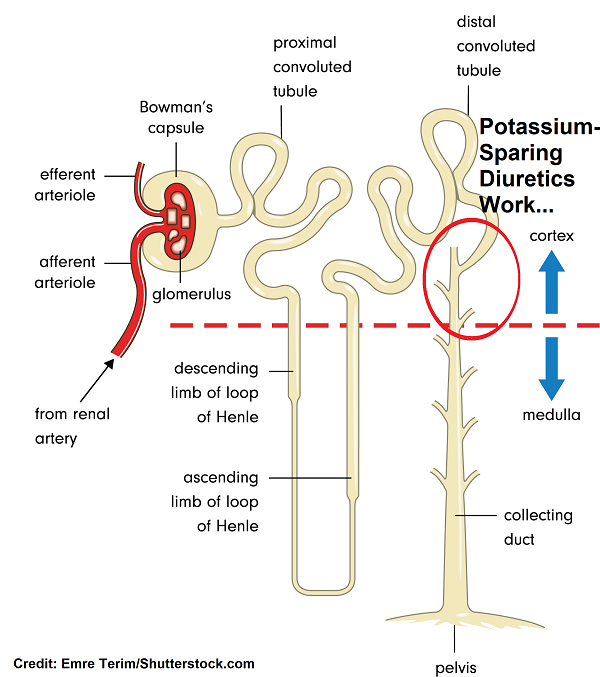
An important concept to remember is that each family of diuretics affect different parts of the nephron. Potassium-sparing diuretics affect the last parts of the nephron (the late part of the distal tubules and collecting duct) in how they deal with sodium and potassium.
Potassium-sparing diuretics can really be divided into two subcategories due to how they work within the nephron to cause diuresis. Each type achieves the same diuretic effect BUT in different ways.
- Epithelial sodium channel (ENac) inhibitors
- Medications in this group include: Triamterene and Amiloride
- These medications directly inhibit the sodium channels within the cells that make up the distal tubule and collecting duct.
How they work to cause diuresis? The sodium channels allow sodium through so it can make its way to the bloodstream (hence to be reabsorbed). Once sodium travels through this channel, it will encounter the sodium- potassium pump where sodium is exchanged for potassium (and hydrogen ions). Then once the sodium is exchanged for potassium it will be reabsorbed back into the bloodstream, and the potassium will enter the filtrate and will be excreted out via the urine. Therefore, this is how sodium is reabsorbed within this section of the nephron. However, these potassium-sparing diuretics directly inhibit the sodium channels so sodium can’t go through it.
Therefore, sodium is not exchanged for potassium via this exchange pump and sodium stays in the filtrate (hence so does water) and this leads to a diuretic effect (the patient will have to urinate more). Furthermore, because the sodium-potassium pump exchange can’t occur, potassium stays in the blood (hence SPARING the potassium, which is why we call them potassium-SPARING diuretics). It’s important to note that some patients can experience HYPERkalemia while taking these medications.
- Aldosterone Antagonists (also called Aldosterone Receptor Blockers)
- Medications in this group include: Spironolactone and Eplerenone
- They work against the role of aldosterone to influence how the sodium channels work.
How they work to cause diuresis? As pointed out above, these medications work against the role of aldosterone within this section of the nephron.
What does aldosterone do? It causes the nephron to reabsorb more sodium and water into the bloodstream but waste potassium. Aldosterone is beneficial in helping increase the blood pressure when it falls too low by increasing the blood volume with the extra sodium and water reabsorbed from the nephron.
Also, aldosterone normally works to influence epithelial sodium channels and sodium-potassium pumps by increasing this number, which causes the reabsorption of sodium into the bloodstream and secretion of potassium into the filtrate.
However, with these medications aldosterone is INHIBITED from influencing these channels and pumps. Therefore, sodium stays in the filtrate (so does water) rather than being reabsorbed back into the bloodstream and potassium stays in the blood rather than being secreted into the filtrate because there is NO exchange happening. Hence, this leads to the diuretic effect.
***Potassium-sparing diuretics are relatively weak in their diuretic effects when compared to the other families of diuretics. This is because of their limited effect on how they alter sodium reabsorption. This why they are sometime prescribed with loop or thiazide diuretics because by combining these diuretics it can help prevent hypokalemia. Remember hypokalemia commonly occurs with loop and thiazide diuretics.
Used for?
- Hypertension
- Edema/swelling due to heart failure, liver impairment, or nephrotic syndrome
- Hypokalemia due to the effects of diuretics that waste potassium
- Hyperaldosteronism (primary aldosteronism or Conn’s Syndrome)…mainly Spironolactone
- This condition occurs when high amounts of aldosterone are produced by the adrenal glands. This causes the body to keep sodium and lose potassium. So, the patient will have hypokalemia and high blood pressure.
- Spironolactone will decrease the amount of aldosterone and help alleviate signs and symptoms of this condition.
Responsibilities as the Nurse?
Patients will be losing fluid in the form of urine: watch for signs of dehydration (removing too much fluid) and electrolyte imbalances (keeping too much potassium in the blood)
- Vitals (elevated heart rate and low blood pressure SBP <90)
- Monitor closely the patient’s intake and output (especially urinary output…avoid in patients with renal failure)
Monitor labs:
- Hyperkalemia: normal potassium is 3.5-5 mEq/L…watch levels >5 mEq/L
- Signs and symptoms of high potassium level: EKG changes tall peaked T waves, muscle weakness/cramps, difficulty breathing, nausea, vomiting, diarrhea, mental status change, paresthesia etc.
- AVOID foods high in potassium or salt-substitutes (they contain potassium)
- Renal function: BUN and creatinine (contraindicated in patient with renal failure)
Administer with a meal or right after to decrease GI side effects.
Monitor CLOSELY if patient is taking:
- ACE Inhibitors, ARBs, or NSAIDs: these medications can increase potassium levels…need to closely monitor potassium level.
- Lithium: potassium-sparing diuretics alter the way the nephron works so they can reduce how well Lithium is cleared from the body, which can lead to lithium toxicity.
- Normal Lithium level is 0.5-1.2 mmol/L
Side effects?
Hyperkalemia, upset stomach, spironolactone: antiandrogen effects (gynecomastia, menstrual irregulars, sexual dysfunction)…this is because spironolactone affects androgen and progesterone receptors
Education Pieces for the Patient?
- Teach patient to be aware of signs and symptoms of dehydration (excessive thirst, fatigue, no urination, hypotension), and hyperkalemia (nausea, vomiting, diarrhea, muscle cramps/weakness, or tingling or paresthesia).
- Limiting foods high in potassium and avoid salt-substitutes:
- Potatoes (pork)
- Oranges
- Tomatoes
- Avocados
- Strawberries
- Spinach
- fIsh
- mUshrooms
- Musk Melons: cantaloupe
References:
Amiloride. Retrieved 20 August 2019, from https://livertox.nih.gov/Amiloride.htm
Food and Drug Administration. Aldactone Spironolactone Tablets, USP [Ebook]. Retrieved from https://www.fda.gov