This is an NCLEX review for pheochromocytoma. Patients who have pheochromocytoma are experiencing excessive amounts of catecholamines in the body due to a tumor. This causes the patient to experience hypertension, tachycardia, hyperglycemia etc. This condition can lead to damage to other systems of the body.
In the previous review, I covered other endocrine disorders. So, if you are studying for NCLEX or your nursing lecture exams, be sure to check out that section.
When taking care of a patient with pheochromocytoma, it is very important the nurse knows how to recognize the typical signs and symptoms seen in these conditions, how it is diagnosed, nursing interventions, and patient education.
Don’t forget to take the pheochromocytoma quiz.
In this NCLEX review, you will learn the following:
Pathophysiology of pheochromocytoma
Causes
Signs and Symptoms of pheochromocytoma
How it is Diagnosed
Nursing Interventions
Treatments
Lecture on Pheochromocytoma
Pheochromocytomas NCLEX Review Notes
pheo: dark chromo: color cyt: cell oma: tumor
Definition: It is a tumor found on the adrenal medulla of the kidneys that secretes excessive amounts of catecholamines.
Pathophysiology of Pheochromocytoma
Key Players:
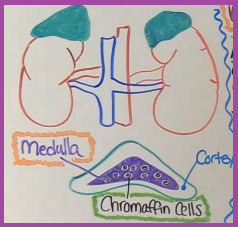 Adrenal gland: the human body has two adrenal glands that are cone-shaped that sit on the kidneys. The outer layer is the adrenal cortex and the center layer is the adrenal medulla (tumors are found here).
Adrenal gland: the human body has two adrenal glands that are cone-shaped that sit on the kidneys. The outer layer is the adrenal cortex and the center layer is the adrenal medulla (tumors are found here).
Adrenal Medulla: found in the adrenal gland and is within the adrenal cortex. Its role is to secrete epinephrine (adrenaline), norepinephrine (noradrenaline), and low amounts of dopamine in response to the body’s sympathetic nervous system (fight or flight system) via chromaffin cells.
Chromaffin Cells: founds in the adrenal medulla and secrete catecholamines. This is what the tumor is made up of (tumors tend to be benign). These cells are also found in the heart, head, neck, bladder, spine, abdomen. If a tumor(s) develops in this area it is known as paragangliomas rather than pheochromocytoma
Catecholamines: have a huge influence on how organs and tissues work. They cause the body to do the following:
- increase heart rate and blood pressure
- increase glucose (stimulates the liver to release it stores of glucose in the blood and blocks the role of insulin)
- increases fat metabolism for energy (breaking down of fats for fuel)
- increases basal metabolic rate (burns more calories)
- increases thermogenesis (elevates body temperature)
- how you respond to stress (example: see a bear…jump and feel fear/anxiety).
—All of this is produced because of stimulation of the sympathetic nervous system in response to fight or flight mechanism and happens normally in the body when stiumalated to do so. However, in pheochromocytoma a patient is experiencing these signs and symptoms due to a tumor.
- Pheochromocytomas wreak havoc the most on the cardiovascular system (due to excessive hypertension).
- Tumor or tumors can be found in one or two glands (most commonly affects one gland).
- Causes…..genetic disposition and commonly found in early to middle aged adults.
Signs & Symptoms of Pheochromocytoma
Remember the mnemonic: Fight & Flight (this helps you remember it is stimulating the sympathetic nervous system & symptoms are going to be extreme)
Facial flushing (from hypertension), fluttering in chest (palpitations)
*Increased blood pressure & heart rate
Glucose high
*Headaches (sudden and severe)
Tremors
*Frequent sweating (from hypertension)
Loss of weight
Increase anxiety and fear
Growing tumor can cause back or abdominal pressure or pain
Heat intolerance
Tired and weak (from the constant stimulation)
*=most common signs and symptoms
***Signs and symptoms can happen in episodes or triggered after an event:
- Eating foods with Tyramine (plays a role in pressure blood): foods that are aged, pickled, fermented like cheeses, red wine, smoke/dried meat, bananas, sauerkraut, chocolate.
- Surgery, trauma injury, emotional stress, medications such as Monoamine Oxidase Inhibitors: MAOIs
Diagnosed
24-hour urine for catecholamines and metanephrines (are metabolites formed when the body breaks down catecholamines)….if too many metabolites are found then there are too many catecholamines being produced). If this test comes back positive the doctor may order a MRI or CT scan of the adrenal glands to inspect for tumors.
Blood test to measure metaneprhines.
Treatment:
- Adrenalectomy: remove the adrenal gland with the tumor (may remove one or both depending on where tumor is located)
- Pre-opt: prescribed alpha-adrenergic blockers
Nursing Interventions for Pheochromocytoma
- Monitor vital signs: blood pressure, heart rate
- Monitor for hypertensive crisis: >180 systolic or >120 diastolic…if blood pressure is too high for a long period of time this can cause damage to vital organs…kidneys, eyes, brain, heart.
- Signs and symptoms of this: headache, vision changes, neuro changes, seizures, shortness of breath
- Monitor for chest pain (risk for MI), neuro status (stroke), EKG changes, hyperglycemia
- Provide a calm and cool environment….no overstimulation!
- Per MD order: Administer pre-opt (prior to adrenalectomy) alpha-adrenergic blockers (Cardura, Minipress, Hyrtin): work by blocking noradrenaline, reduces catecholamines. These medications help decrease blood pressure and prevent a hypertensive crisis during surgery.
- Alpha-adrenergic blockers can cause reflex tachycardia (due to the decrease in blood pressure). The heart rate increases in an attempt to increase the blood pressure as a “reflex” response, and these medications can causes orthostatic hypotension.
- Doctor may also be prescribe patient a beta-adrenergic blockers like Labetalol or Inderal to help with hypertension and tachycardia
Education for patient with pheochromocytoma:
- Eat high calorie diet: burning fats at a rapid rate
- Avoid stimulant substances: energy drinks, caffeine products, or smoking (due to vasoconstriction)
- For patient going for an adrenalectomy: educate about having to take hormone replacement medications after surgery and taking alpha-adrenergic prior to surgery (usually 2 weeks before surgery)
- If patient is having a bilateral adrenalectomy (both glands removed ): will have to take glucocorticoids and mineralocorticoid for life.
- If patient is having a unilateral adrenalectomy (only one gland removed): will have to take glucocorticoids for approximately 2 years.
More NCLEX Reviews
References
- Pheochromocytoma and Paraganglioma Treatment. (2016). National Cancer Institute. Retrieved 20 November 2016, from https://www.cancer.gov/types/pheochromocytoma/patient/pheochromocytoma-treatment-pdq