This NCLEX review will discuss bone fractures.
As a nursing student, you must be familiar with bone fractures, along with how to care for a patient experiencing one.
These type of questions may be found on NCLEX and definitely on nursing lecture exams.
Don’t forget to take the bone fractures quiz.
You will learn the following from this NCLEX review:
- Definition of bone fractures
- Types
- Signs and Symptoms
- Complications
- Nursing Interventions
- Treatment
Bone Fractures NCLEX Review Lecture
Bone Fracture NCLEX Review
What is a bone fracture? It’s a break or crack in a bone.
Causes of Bone Fractures: happens because the bone can NOT withstand the force
- Trauma (fall, car accident etc.)
- Twisting (sports injury, abuse etc.)
- Diseases (bone cancer or osteoporosis)
Children tend to heal faster than adults from bone fractures because the periosteum (the dense fibrous membrane covering the bones) is stronger, more flexible, and thicker than an adults.
It can take anywhere from 3 to 12 weeks to heal from a bone fracture, depending on the person’s age and health status.
Complications of a bone fracture include:
- Infection (osteomyelitis)
- Compartment syndrome
- Fat embolism
Signs and Symptoms of a Bone Fracture
“BROKEN”
Bruising over the site (discolored with swelling) and pain
Reduced movement of extremity or muscle
Odd appearance (looks abnormal)
Krackling sounds due to bone fragments rubbing together (crepitus)
Edema and erythema at the site
Neurovascular impairment…6 P’s (ischemia: pain, pallor, paralysis, paresthesia, pulselessness (late sign), poikilothermia)
Types of Bones Fractures:
**Remember these types!!
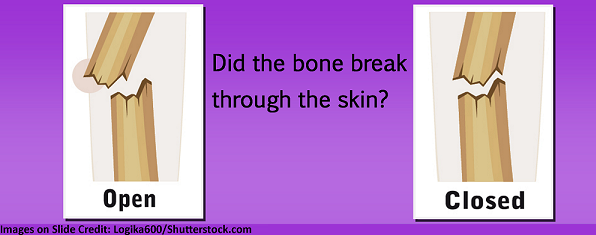
- Did it break through the skin? Open or closed
Open Fracture (“Compound”): a fractured bone that breaks through the skin
Closed Fracture (“Simple”): a fractured bone that does NOT penetrate through the skin (skin remains intact)

- Is the bone completely broken or part of it? Complete or incomplete
Complete Fracture: the fracture completely separates the bone in two
Incomplete Fracture: the fracture does NOT break the bone all the way through

- What is the pattern or details or the fracture? Straight across, up and down, at an angle, crushed in fragments
Greenstick: one side of the bone is bent while the other is broken…incomplete type of fracture (most common in pediatric patients because their bones are more flexible than an adults)
Comminuted: the bone is broken into many fragments (3 or more)

Transverse: the fracture is straight across the bone shaft
Oblique: the fracture is slanted across the bone shaft

Spiral: the fracture twists around the bone shaft (from a twisting injury)
Nursing Interventions for Fractures
- After a fracture confirm the patient is safe (out of harm’s way) and stable then…..
- Immobilize the fracture by using a device to splint it: (it keeps the patient from using the affected extremity)
- WHY is this important to do? The goal is to help a bone fracture heal properly by putting it back in its original state (if it moves this can cause improper healing). In addition, it prevents more surrounding tissue damage, bleeding, and pain.
- Stop bleeding, if present, by applying pressure with a clean cloth (be sure you know if your patient takes blood thinners, and if possible, what their PT/INR (Coumadin) and PTT (Heparin) values are.
- If the fracture is an opened “compound” fracture, cover with sterile dressing!
- Elevate extremity to decrease swelling.
- Apply ice wrapped in towel to the injury to decrease swelling (want to prevent excessive swelling due to the risk of compartment syndrome).
- Keep NPO (nothing by mouth) until evaluated by surgeon…may need surgery.
- X-ray will be ordered to diagnose a possible fracture and what type.
- Pain management with prescribed medications: document and closely monitor how the medication is relieving the pain…very important!! Watch out for compartment syndrome (pain is not relieved with medication and it hurts with passive movement like stretching or elevating the extremity).
- Monitor for fat embolism , especially if this is a long bone fracture: Assess mental status and respiratory system: confusion, restless, increased respiration, difficulty breathing
- Assess neurovascular status! Assess the 6 P’s: this assesses the function of the nerves and blood flow for possible compartment syndrome (if not caught early this will lead to IRREVERSIBLE nerve, muscle, damage and tissue death)
- Immobilize the fracture by using a device to splint it: (it keeps the patient from using the affected extremity)
What is Compartment Syndrome?
Compartment syndrome occurs when too much pressure is exerted within the muscle compartments found within t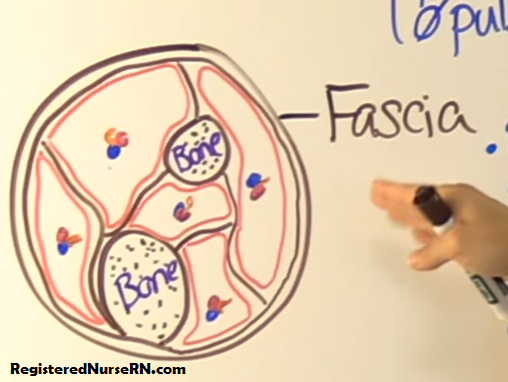 he fascia.
he fascia.
This can occur when there is hemorrhaging (bleeding) or swelling present after an injury, like with a bone fracture (or with external factors like a cast being too tight or traction). All this can increase the pressure within the compartments. As the pressure builds, this will cut off the blood supply and nerve function to this muscle. If not corrected within 6 hours, the damage is permanent.
Remember from anatomy and physiology that in the leg and arm there are individual compartments grouped together (but separated from one another) that contain bone, muscle, nerves, and vessels. Each compartment usually has it own muscle, nerve, and vessel supply. Fascia is what keeps all these structures in place and separated.
The important thing to remember about fascia when talking about compartment syndrome is that is does NOT expand when pressure increases within a compartment (so there will be no relief within the compartment from the fascia).
Instead the pressure stays within the compartment and causes blood vessel and nerve function to become compromised (diminished). So, ischemia is going to occur to the muscle and distal extremity to the fracture.
Assess the 6 P’s:
- Pain (early sign)
- Paresthesia (can be an early sign too)
- Pallor
- Paralysis
- Poikilothermia
- Pulselessness (late sign)
Pain: worst with passive touch or movement, elevating the limb, or any pressure, stretching increases the pain. Pain medication is not relieving it.
Paresthesia: patient may report it feels like the extremity distal to the fracture feels like it is falling asleep or a “pin and needle” sensation. Can they feel you touch their extremity? ALWAYS CHECK THE UNAFFECTED EXTREMITY TO COMPARE!
Pallor: Extremity should be pink and have normal capillary refill less than 2 seconds. In CS, it may appear pale or dusky and have a capillary refill greater than 2 seconds. ALWAYS CHECK THE UNAFFECTED EXTREMITY TO COMPARE!
Paralysis: can the patient move the distal extremity from the fracture or has the movement decreased…this is a bad sign! ALWAYS CHECK THE UNAFFECTED EXTREMITY TO COMPARE!
Poikilothermia: This occurs when the affected extremity distal from the fracture feels cooler to the touch compared to the unaffected extremity. The extremity can NOT regulate its temperature.
Pulselessness: Always mark the pulses with a black marker and have a Doppler available to monitor the sound of the pulse. (this is a late sign in compartment syndrome)
Nursing interventions for Compartment Syndrome:
- keep the extremity AT HEART level (NOT below….remember you want to maintain arterial pressure and elevating it above heart level will cause more ischemia)
- loosen and remove restrictive items
- notify the physician
- perform neurovascular checks (6 P’s)
- prepare the patient for possible bivalvement of the cast, reduction of weight in the traction, or in severe cases fasciotomy.
Various treatments for a Bone Fracture:
Bone reduction: putting the fractured bone back in its original state.
Closed reduction: done manually….nonsurgical with general anesthesia
- Cast (plaster or fiberglass) placed to keep broken bone in place to allow it to heal
Things to remember about casts:
- Monitor for compartment syndrome: 6 P’s
- Monitor for infection: hotspots in the cast, severe pain, fever
- Keep the cast and extremity elevated above the heart level (decreases swelling)
- Apply ice packs to the cast for the first 2 days to decrease swelling
- Even drying for new cast by turning every 2 hours
- Use palms of hand to handle (not fingertips) with a new wet plaster cast.
- WHY? Prevents dent formation in the cast by handling with the palms of hand, which can cause skin breakdown overtime.
- Maintain skin integrity: petal the cast….. use soft tape called moleskin around the edge to prevent skin breakdown
- Keep cast dry and never stick anything inside to scratch an itch
Open reduction: done surgically to put fractured bone back in its original state and a fixation device used:
- Internal: attached to the bone inside the skin (pins, rods, plates, screws or external)
- External: fixture attached to the outside of the skin that helps with bone healing (can be adjusted…metal braces, screws)
Traction: aligns the bone with a constant steady pulling action.
- Make sure the weights are hanging freely and not on floor
- Never remove weights with a MD order
- Pin care and monitor for infection (odorous draining, redness, pain)
- Neurovascular status: 6 P’s
- Overhead trapeze bar to move around in bed
References:
- Assessment & Initial Management of the Trauma Patient. (2006). Emergency.cdc.gov. Retrieved 3 October 2017, from https://emergency.cdc.gov/masscasualties/word/blast_curriculum_3H.doc
- Cast Care | HealthReach. HealthReach. Retrieved 4 October 2017, from https://healthreach.nlm.nih.gov/document/546/Cast-Care