This NCLEX review will discuss myasthenia gravis.
As a nursing student, you must be familiar with this neuro disease along with how to provide care to a patient experiencing this condition.
Don’t forget to take the myasthenia gravis quiz.
You will learn the following from this NCLEX review:
- Definition of myasthenia gravis
- Pathophysiology
- Signs and Symptoms
- Nursing Interventions
- Medications
- Treatments
Myasthenia Gravis NCLEX Lecture
Myasthenia Gravis NCLEX Review
What is Myasthenia Gravis? It’s an autoimmune condition where the body attacks the receptors that allow for voluntary muscle control, which leads to muscle weakness.
What voluntary muscles are involved?
- Eyes: most likely will be the first sign something is wrong
- Throat: another common sign…hoarse voice and problems swallowing
- Face
- Arms/Legs
- Respiratory muscles for breathing (in severe cases)
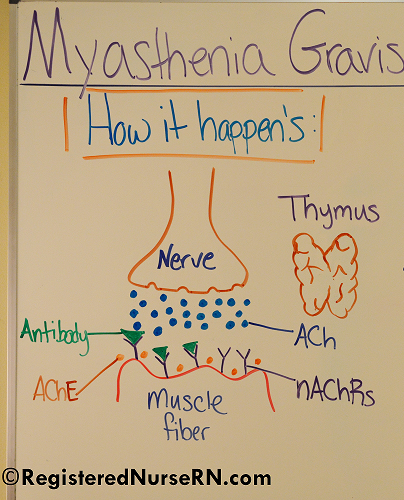
How does Myasthenia Gravis happen?
 Key Players Involved:
Key Players Involved:
Neuromuscular Junction:
- Nicotinic Acetylcholine Receptors (NAChRs) or the function of Muscle-Specific Kinase (MuSK). MuSK helps with maintaining and building the neuromuscular junction, but for this lecture we will concentrate on the nicotinic acetylcholine receptors.
- Neurotransmitter: Acetylcholine
- Immune System: produces the anti-bodies against the nicotinic receptors.
- Thymus gland
- Acetylchoinesterase: an enzyme that breaks down acetycholine (remember this substance because it plays a role in the treatment of MG with anticholinesterace medications).
In myasthenia gravis the issue arises at the neuromuscular junction. This is the place where the motor neuron and muscle fiber meet and the neurotransmitter acetylcholine is released.
At this junction are receptors on the muscle fiber called nicotinic acetylcholine receptors that become stimulated when acetylcholine is released and cause contraction of the muscle fiber.
However, in myasthenia gravis the nicotinic acetylcholine receptors are being attacked by antibodies the immune system has created and are not working properly. These receptors can NOT access the release of acetylcholine and cause muscle contraction, so there is muscle weakness.
The thymus gland (found anteriorly in the upper part of the chest behind the sternum in between the lungs) plays a very important role in our immune system health. It’s the creator of T-cells, which are super important for immune health by fighting viruses and bacteria.

In children the thymus is large (remember it will produce most of the body’s T-cells by the time a person attains puberty). It should shrink by adulthood and then in older age be like a fatty tissue. But in people with myasthenia gravis, the thymus gland tends to stay large and develops tumors or collection of immune cells in the gland. It is thought that the thymus erroneously causes immune cells to produce antibodies that will attack receptor sites on these voluntary muscle neuromuscular junctions.
Signs and Symptoms of Myasthenia Gravis
**HALLMARK: muscle weakness becomes worse with activity (especially repetitive activity) but will improve after resting the muscle.
Patients tend to notice symptoms in the eyes due to eye muscle weakness of the extraocular muscles or have problems with speaking (slurred) or swallowing….signs and symptoms vary among patients.
“WEAKNESS”
Weakness neck, face, arms/legs/hands
Eyelid drooping…can be one eye or both (Ptosis)

Appearance mask-like: no expression…looks very sleepy
Keeps choking or gagging when eating (difficulty swallowing)…many muscles help with the swallowing process and have become weak
No energy…very fatigued…gets worse throughout the day as muscles are used
Extraocular muscle involvement leading to double vision…strabismus

Slurred speech (voice may be hoarse and very soft)
Short of breath (can extend to respiratory muscles)
Complications of Myasthenia Gravis
Myasthenia gravis can go into remission where the patient doesn’t have signs and symptoms, but some patients can experience severe acute exacerbation with a complication called Myasthenic Crisis. This is where the disease is becoming worse and the patient may need intubation and mechanical ventilation to breathe.
Risk factors for experiencing Myasthenic Crisis: improper dosage (not enough) of anticholinesterase meds to treat this condition, stress (physical…surgery or mental), and respiratory infection.
That patient will have severe weakness of muscles that cause respiratory failure.
How is it diagnosed?
- UPDATE: Tensilon test is no longer used in the US. The FDA discontinued edrophonium in 2018 due to a high rate of false positives.
- Edrophonium (Tensilon test): During this test a medication is given called edrophonium.
- How does the medication work? It prevents the breakdown of acetylcholine at the neuromuscular junction, which allows more of the neurotransmitter to be present at the neuromuscular junction.
- It is used to diagnose Myasthenia Gravis AND differentiate between a myasthenic crisis and cholinergic crisis (see more about cholinergic crisis in the pharmacology part of this lecture).
IMPORTANT:
What will happen if Edrophonium is given to a patient with myasthenia gravis or to a patient in myasthenic crisis? The patient’s signs and symptoms will temporarily improve. Hence, the test is positive.
What will happen if Edrophonium is given to a patient with cholinergic crisis? The patient’s signs and symptoms will become worse….NO improvement. Hence, the test is negative.
- If this happens the nurse (per MD order) will administer the antidote for Edrophonium, which is ATROPINE! It is also important to have the patient on a cardiac monitor during the test and a crash cart within reach if an emergency arises.
Nursing Interventions & Medications for Myasthenia Gravis
Monitor respiratory status: effort of breathing, respiratory rate, oxygen saturation, does the patient feel like it’s hard to breathe? If hospitalized with exacerbation needs resuscitation equipment close by: suction etc.
Monitor neuromuscular status:
- Assessing vision (double vision?), quality of voice, swallowing (important for medication administration…ALWAYS check swallowing before giving meds), facial appearance, strength with arms/legs, cranial nerves
Safety: at risk for injury….needs assistance at all times (remember the patient may have double vision (eye patch to help with this), arm and leg weakness)
Speech pathologist will evaluate and recommend treatment based on findings. Patient may need or have a feeding tube and you will be managing this as the nurse.
Monitor for aspiration, hob of greater than 30′ while eating
Education about food because patient may have difficulty chewing and swallowing:
- smaller meals that are easy to chew foods…pick food options that are soft and require minimal effort to chew
- try scheduling meals during peak time of medication (30 minutes to 1 hour before eating) so chewing and swallowing muscle will have the most access to acetylcholine
- Thicken liquids for swallowing
- Take small bites and rest while eating and before a meal
- It’s best to have large meals at the beginning of the day than at the end (remember patients with MG becomes progressively weaker throughout the day)
Educate about performing most of their activities early in the day when the patient will have the most energy.
Help patient identify things that makes symptoms worst: menstrual cycle, sickness, stress, extreme temperatures
Medications for Myasthenia Gravis:
Anticholinesterase: “Pyridostigmine” …improves symptoms…there is no cure!
How does the anticholinesterase medication work? Remember the substance we talked about earlier called acetylcholinesterase? This medication will prevent it from working. Therefore, there will NOT be the breakdown of acetylcholine. Therefore, more of it will be available at the neuromuscular junction site. This will help improve muscle strength.
Patient should take 30 to 60 minutes before a meal to help increase muscle strength with swallowing and chewing.
Monitor: Myasthenic crisis (from not enough medication) or cholinergic crisis (too much of the medication): ….both will have respiratory failure and severe muscle weakness but from different causes.
Signs and Symptoms of Cholinergic Crisis:
Think of the signs and symptoms experienced during cholinergic crisis similar to the parasympathetic nervous system being in overdrive:
- Pupil constriction
- Bronchoconstriction….eventually respiratory failure
- Increased salivation and mucous production
- GI problems: abdominal cramping, vomiting, diarrhea
- Bladder incontinence
- Bradycardia
Treatment: No anticholinesterase medications and atropine to reverse symptoms.
Other drugs used to treat MG: corticosteroids and immunosuppressants
Other treatments for MG:
- Thymectomy: removal of the thymus gland (improves symptoms in some patients…NOT a cure)
- Plasmapheresis with administration of IV immunoglobulins (severe cases): filters blood by removing antibodies that attack the receptors at the neuromuscular junction (temporary improvement for about 4 weeks to a couple of months….NOT a cure).
References:
- Myasthenia Gravis Fact Sheet | National Institute of Neurological Disorders and Stroke. Ninds.nih.gov. Retrieved 27 November 2017, from https://www.ninds.nih.gov/Disorders/Patient-Caregiver-Education/Fact-Sheets/Myasthenia-Gravis-Fact-Sheet
- Recognition of Illness Associated With Exposure to Chemical Agents-United States, 2003. (2003) (p. 939). Retrieved from https://www.cdc.gov/nceh/hsb/chemicals/pdfs/mmwr5239p938.pdf