This abnormal rhythm originates from the electrical components within the AV junction, such as the AV node or the bundle of His. These structures exhibit increased automaticity, causing them to fire more quickly than usual. However, the primary pacemaker of the heart, the SA node, is unable to function as the main conductor due to either being too slow or not working. In turn, the structures in the AV junction assume control.
Junctional tachycardia is a type of SVT (supraventricular tachycardia) because it originates above the ventricles.
Check out the lecture on junctional tachycardia rhythm below and don’t forget to take the free review quiz on junctional tachycardia when you’re done reviewing this material.
ECG/EKG Study Guide and Workbook for Nursing Students
“ECG/EKG Interpretation Study Guide and Workbook by Nurse Sarah”. This book contain 100 pages of content featuring 26 ECG rhythm break downs, 51 ECG rhythm analysis practice problems, 100 comprehensive ECG practice questions, worksheets, chart summaries, and more.
You can get an eBook version here: “Nurse Sarah ECG Book” or a physical copy here: “ECG/EKG Interpretation Study Guide by Nurse Sarah“.
So how is this rhythm going to appear?
In normal electrical conduction, the SA node initiates the signal, which travels down to the AV node, then the bundle of His, followed by the bundle branches (right and left), and finally, the purkinje fibers. This sequence results in the formation of the PQRST waveform on the ECG.
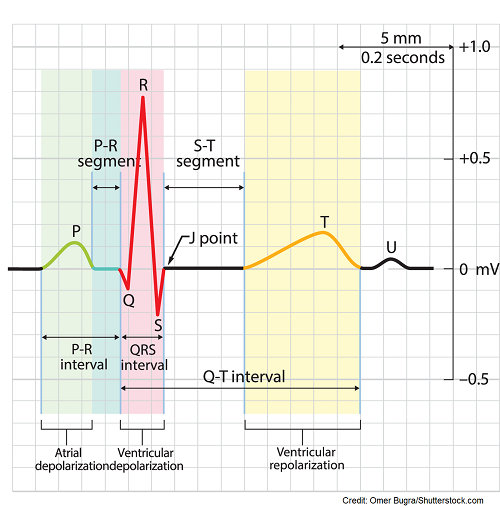
You should see one p wave in front of one QRS complex, normal PR interval 0.12-0.20 seconds, normal QRS, QT interval, and T wave
What is happening in junctional tachycardia?
The SA node is NOT the main conductor anymore, the AV junction structures (usually the AV node) is the primary pacemaker now. These structures are sending out signals really fast. These fast signals will go down through the ventricles normally, which create a narrow QRS complex <0.12 seconds, normal QT interval and t wave. Therefore, the ventricular rate (R to R measurement) will be regular.
However, the electrical signals will go up through the atria (rather than down), hence retrograde, and this affects how the P waves will appear on the ECG.

Key Characteristics to remember:
- Rate >100 bpm and regular
- QRS narrow <0.12 seconds, normal QT interval and T wave
- P waves abnormal and appear upside down (inverted) in leads II, III, aVf
- The p wave can be found in any of these places:
- concealed (hiding in the QRS complex)
- behind the QRS complex…no PR interval in this case
- before the QRS but be very close to it leading to a short PR interval <0.12 seconds
- The p wave can be found in any of these places:
Jingle to remember:
Inverted P on aVF, 2, and 3,
Before or after QRS, if you can see.
Sometimes it hides, and you can’t see it at all,
but when it appears in the front, the PR interval is small.
Causes of Junctional Tachycardia:
Rare occurrence in adults but can be caused by a myocardial infarction, heart muscle inflammation, or digoxin toxicity. More common in pediatric population with congenital heart issues post-heart surgery.
Nursing’s Role:
Check for symptoms that suggest a decrease in cardiac output. When the heart beats at a very fast rate it does not fill properly and it pumps out less blood. This leads to a decrease in cardiac output.
Monitor for signs and symptoms of low cardiac output: shortness of breath, low blood pressure, dizziness, chest pain, increased capillary refill >2 seconds, weak pulse etc.
Medications to slow down the rate: beta-blockers, calcium channel blockers like diltiazem or verapamil, or antiarrhythmics like flecainide. If this doesn’t work, a cardiac ablation can be performed to to destroy the tissue that is causing the abnormal rhythm.
References:
Hafeez Y, Grossman SA. Junctional Rhythm. [Updated 2023 Feb 5]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK507715/
How the Heart Works | NHLBI, NIH. Retrieved 15 February 2022, from https://www.nhlbi.nih.gov/health-topics/how-heart-works
Page, R, Joglar, J, Caldwell, M. et al. 2015 ACC/AHA/HRS Guideline for the Management of
Adult Patients With Supraventricular Tachycardia: Executive Summary: A Report of the
American College of Cardiology/American Heart Association Task Force on Clinical Practice
Guidelines and the Heart Rhythm Society. J Am Coll Cardiol. 2016 Apr, 67 (13) 1575–1623.
https://doi.org/10.1016/j.jacc.2015.09.019
Thaler, M. S. (2010). Arrhythmias of Sinus Origin. In The Only EKG Book You’ll Ever Need (6th ed., pp. 110–111). essay, Lippincott, Williams, Wilkins.