This abnormal rhythm occurs when the primary pacemaker of the heart (SA node) functions too slowly or malfunctions. Consequently, alternative pacemaker structures located in the AV junction of the heart initiate the heartbeat. These structures serve as a backup, preventing the heart from entering cardiac standstill, as they step in when the SA node fails to function properly.
The AV junction in the heart acts as a divide between the atria and ventricles, housing electrical components such as the AV node and bundle of His.
Check out the lecture on junctional escape below and don’t forget to take the free review quiz on junctional escape when you’re done reviewing this material.
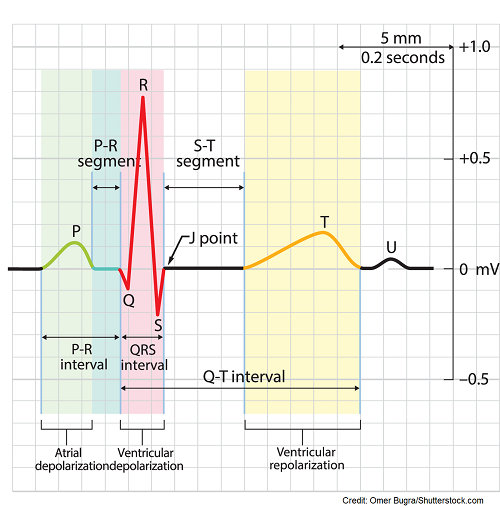
To comprehend junctional rhythms, let’s briefly revisit the typical path of electrical conduction in the heart that generates the PQRST waveform on an ECG:
The electrical signal typically originates in the SA node situated in the upper section of the right atrium, acting as the primary pacemaker of the heart and regulating a heartbeat of 60-100 bpm. When activated, it transmits electrical signals downwards across the atria, triggering depolarization in the cells of both the right and left atrium, resulting in their contraction. Consequently, this produces a distinctive upright and easily visible P wave preceding each QRS complex.
Then, the electrical signals proceed to the:
- AV node (atrioventricular node): located in the lower part of the right atrium just above the tricuspid valve, this node acts as the heart’s “gatekeeper.” It serves as a backup pacemaker and can take control if the SA node is sluggish or malfunctioning, regulating the heart rate to 40-60 bpm.
- The AV node is recognized for introducing a delay in electrical signaling to allow the atria time to empty blood into the ventricles. Without this delay, incomplete blood emptying from the atria to the ventricles could lead to complications.
- Then it’s time for the ventricles to be depolarized (hence contract). The electrical signal travels down to the bundle of His (the third type of pacemaker beating around 20-40 bpm).
- Next, the signal branches off into the bundle branches (right and left).
- Finally, the signal reaches the Purkinje fibers, leading to ventricular depolarization. This creates the QRS complex.
- Following this, repolarization takes place creating the T wave, and the cycle repeats continuously.
Result if everything is firing as it should:
Normal ecg waveform with one upright P wave in front of one QRS complex, normal PR interval 0.12-0.20 second, normal QRS complex <0.12 second, normal QT interval and T wave.
What’s happening in junctional escape rhythm:
The SA node, which typically acts as the primary pacemaker, is either too slow or not functioning properly. Consequently, the rhythm shifts to originate from the AV junction, such as the AV node or bundle of His, which serve as backup pacemakers of the heart and take over by transmitting signals.
These signals exit the AV node and proceed down through the ventricles as usual, resulting in a normal QRS complex, QT interval, and T wave. However, electrical signals also travel upward (retrograde) through the atria, opposite to their usual direction. This significantly alters the appearance of the P wave and its position on the ECG waveform, providing key insights into understanding junctional rhythms.
ECG/EKG Study Guide and Workbook for Nursing Students
“ECG/EKG Interpretation Study Guide and Workbook by Nurse Sarah”. This book contain 100 pages of content featuring 26 ECG rhythm break downs, 51 ECG rhythm analysis practice problems, 100 comprehensive ECG practice questions, worksheets, chart summaries, and more.
You can get an eBook version here: “Nurse Sarah ECG Book” or a physical copy here: “ECG/EKG
Key characteristics you are looking for when analyzing this rhythm:

- Rate is regular (r to r, ventricular rate regular)
- Rate is 40-60 bpm
- if rate 60-100 bpm, it’s accelerated junctional rhythm
- if rate >100 bpm, it’s junctional tachycardia
- QRS complex will be narrow <0.12 seconds
- QT interval normal and T wave normal
- P wave and PR interval will be abnormal:
- **P waves abnormal (can be any of these):
- appear upside down (inverted) in leads II, III, aVf
- concealed (hiding in the QRS complex) or behind the QRS complex…no PR interval in this case
- before the QRS but be very close to it leading to a short PR interval <0.12 seconds
- Appear upside down (inverted) in leads II, III, aVf
- **P waves abnormal (can be any of these):
Causes of Junctional Escape:
- Sick sinus syndrome occurs when the sinoatrial node (the primary pacemaker) is damaged.
- Cardiac damage can be caused by conditions like myocardial infarction, inflammation of the heart muscle or its lining
- Medications such as digoxin toxicity, beta blockers, calcium channel blockers, and lithium can also affect the heart’s rhythm.
- It is normal for athletic individuals or young children, especially during sleep.
Nursing’s Role and Treatment:
Assess for symptoms:
- Do they exhibit any symptoms?
If not, continue monitoring without the need for treatment.
Monitor for signs and symptoms of low cardiac output, such as:
- Shortness of breath
- Low blood pressure
- Dizziness
- Chest pain
- Increased capillary refill time
- Weak pulse
These symptoms may manifest when the heart rate falls below 60 bpm, as many patients can’t manage a low heart rate and uphold cardiac output.
Check for any medications that could cause this: digoxin, beta blockers, calcium channel blockers, lithium etc.
Treatment is similar to symptomatic bradycardia and involves:
- Addressing the underlying causes by discontinuing or providing antidote medications if needed
- Administering Atropine to elevate heart rate and cardiac output
- Using a temporary pacemaker
- Considering a permanent pacemaker
References:
Hafeez Y, Grossman SA. Junctional Rhythm. [Updated 2023 Feb 5]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK507715/
How the Heart Works | NHLBI, NIH. Retrieved 15 February 2022, from https://www.nhlbi.nih.gov/health-topics/how-heart-works
Thaler, M. S. (2010). Arrhythmias of Sinus Origin. In The Only EKG Book You’ll Ever Need (6th ed., pp. 110–111). essay, Lippincott, Williams, Wilkins.