Anaphylactic shock nursing NCLEX review for students!
In this review, you will learn about anaphylactic shock.
After reviewing these notes, don’t forget to take the quiz that contains anaphylactic shock NCLEX questions and to watch the lecture.
Lecture on Anaphylactic Shock
Anaphylactic Shock NCLEX Review
What is anaphylactic shock? It occurs due to the introduction of an allergen in the body. This leads to mast cells or basophils to release histamine and other chemicals system-wide. This will decrease tissue perfusion causing shock to occur.
Anaphylactic shock is a form of distributive shock. The other types distributive shock are neurogenic and septic shock.
How does an allergen enter the body to cause anaphylactic shock? An allergen can enter various ways such as via an: injection, inhalation, oral, or contact with the skin.
Known Substances that can cause Anaphylactic Shock:
- Foods (shellfish, peanuts, eggs, milk)
- Medications (vaccines, contrast dye, NSAIDS, antibiotics…Penicillin)
- Insect venom
- Latex
- Physical exercise
- Unknown cause: “idiopathic”
Now, let’s talk about what is occurring during anaphylactic shock, and to do this we need to talk about the two types of reactions that can lead to anaphylactic shock.
Anaphylactic shock can occur either due to an immune response where IgE antibodies are created or due to a non-immune response. Regardless of the reaction, both cause the same signs and symptoms, and occur because mast cells or basophils release histamine and other mediators.
- Anaphylactic reaction
- IgE related (immunological):
- Patient has to experience sensitization for reaction to occur!
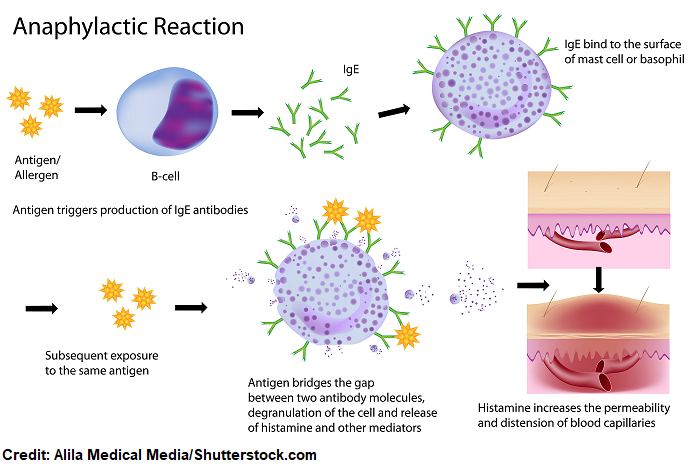
- Sensitization is where the patient has a first-time exposure to an allergen that causes the creation of IgE antibodies. The antibodies attach to the mast cell or basophil and hang out waiting for the second exposure. When the second exposure to the allergen occurs, it causes the mast cells or basophils to release histamine and other substances. This leads to the anaphylactic reaction.
- It’s a Type I Hypersensitivity Reaction: This means the allergen attaches to immunoglobulin E (IgE) antibodies (these antibodies are created due to this allergen) on mast cells and basophils. This leads to a system-wide release of histamine and other mediators…..this is illustrated below.
- Anaphylactoid reaction
- Non-IgE related (non-immunological):
- The patient doesn’t have to be sensitized for the reaction to happen….but can happen with the first-time exposure.
- Causes same reaction as anaphylactic, but it’s not via the immunoglobulin IgE antibodies on the mast cells or basophils.
- Allergens for this type of reaction include: contrast dyes, chemotherapy agents, NSAIDS, etc.
- These agents directly cause the mast cells and basophils to breakdown and release histamine.
- Allergens for this type of reaction include: contrast dyes, chemotherapy agents, NSAIDS, etc.
Effects of Histamine on the Body during Anaphylactic Shock
Histamine will cause:
- Dilatation of vessels (lowers blood pressure and tissue perfusion)
- Bronchoconstriction (narrow airways and respiratory failure)
- Increases heart rate
- Increases the permeability of vessels (leads to swelling and depletes intravascular space of fluid that shifts to the interstitial space)
- Itching
- Increases contraction of GI stomach muscles and increases gastric secretions (leads to nausea, vomiting, diarrhea, and GI pain)
It affects the following systems of the body: Cardiac, Respiratory, GI, and Skin
Signs and Symptoms of Anaphylactic Shock
The signs and symptoms of anaphylactic shock occur mainly due to histamine. So if you remember the effects of histamine on the body during anaphylactic shock, the signs and symptoms are easy to recall.
Respiratory: dyspnea, wheezing (bronchoconstriction), swelling of upper airways due to edema “tightness”, can’t speak, coughing, stuffy nose, watery eyes
Cardiac: tachycardia, hypotension (vasodilation)…may lose consciousness or become dizzy
GI: vomiting, nausea, diarrhea pain
Skin: red, swollen, itchy, hives (vasodilation)
Nursing Interventions and Treatments for Anaphylactic Shock
Prevention! Know your patient’s allergies (assess, document, and AVOID patient’s allergens). Anytime the patient is started on a new mediation or needs a procedure that requires something that is known as an allergen, always go back and review the patient’s allergies!
Implement your hospital’s prevention measure system for allergens by using signs or bracelets for the patients with allergies. This will help make sure other members of the health care team aware of the patient’s allergies as well.
Remember anaphylactic shock can start occurring with seconds to minutes of the exposure.
Recognize the signs and symptoms and ACT FAST!
Allergen (remove it) & Airway (manage airway with high flow oxygen and continuous vital sign monitoring)
Call Rapid Response (start CPR, if needed, until help arrives)
Trendelenburg Position: this is the supine position with the legs elevated (unless vomiting (lay on side) or having major airway issues). This position will help increase venous return to the heart and increase cardiac output and blood pressure.
 First-line Drug is Epinephrine: This medication can administered IM or Subq (dose may be repeated, if needed per MD order). It may needed IV if severe hypotension persists. Epinephrine causes vasoconstriction which will increase the blood pressure, reduce swelling, and cause bronchodilation.
First-line Drug is Epinephrine: This medication can administered IM or Subq (dose may be repeated, if needed per MD order). It may needed IV if severe hypotension persists. Epinephrine causes vasoconstriction which will increase the blood pressure, reduce swelling, and cause bronchodilation.
Administer other medications per MD order (these medications may be ordered depending on the patient’s status): IV fluids, breathing treatment of Albuterol, Antihistamines to target H1 (Diphenhydramine) and H2 (Ranitidine), Corticosteroids to prevent a recurrent attack
Stay and monitor patient very closely: at risk biphasic anaphylaxis (signs and symptoms occur again even if not exposed to allergen…can happen hours after initial attack…may be less, worst, or the same as initial attack)
TEACH!!!
- Patient education:
- Importance of avoiding allergen (may need allergy tests)
- Wearing medical alert bracelets and letting others know about allergen. Example: a child’s caregiver, teacher, friends etc.
- ALWAYS carry an Epi-Pen! It’s administered in the middle of the outer thigh.
- Replace when expired.
- Have patient demonstration how to use (there are Epi-Pen Trainer devices that can assist with this teaching):
- It’s an auto-injector.
- Administered in the middle of outer thigh (can do this through clothes, if needed).
- After injecting the needle, hold the device in place for 3 seconds, so medication is fully injected and then remove.
- Massage the injection site for 10 seconds after injection. This will increase absorption.
- Seek medical attention immediately!
References:
Mylan. How to Use an EpiPen (Epinephrine Injection, USP) Auto-Injector [Ebook]. Retrieved from https://www.epipen.com/-/media/files/epipen/howtouseepipenautoinjector.pdf