Fetal heart tone (FHT) monitoring helps assess how a baby is tolerating labor. It provides information about oxygenation and overall fetal status.
There are two main ways to monitor fetal heart tones:
Methods of Fetal Heart Monitoring
1. Internal Monitoring
- A spiral electrode is inserted through the cervix and attached to the baby’s scalp
- Advantages: Very accurate and reliable
- Disadvantages: Invasive to both mother and baby
2. External Monitoring
- An ultrasound transducer is placed on the mother’s abdomen
- Advantages: Noninvasive
- Disadvantages: Less reliable than internal monitoring and may be affected by fetal position
Quiz & Video on Fetal Heart Tone Decelerations
After you read this article, be sure to take a Fetal Heart Tone Quiz and test your knowledge on this material.
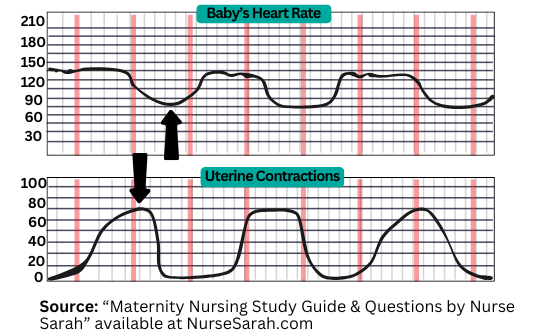
How to Read the Fetal Monitoring Strip
When looking at the monitor, you will typically see:
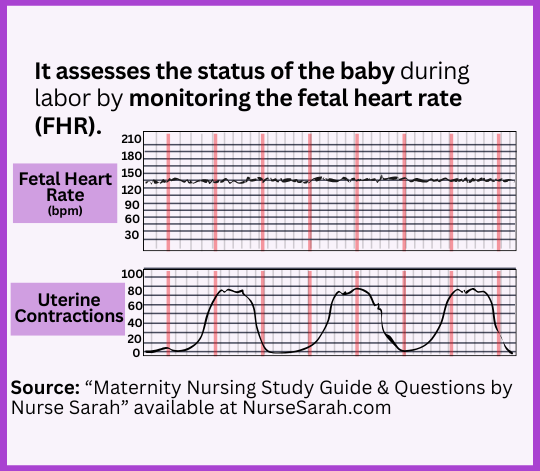
Top Strip: Fetal Heart Rate (FHR)
- Displays the baby’s heart rate
- A squiggly line shows how the heart rate is trending
- Numbers on the side indicate heart rate ranges
- Normal baseline FHR: 110–160 beats per minute (bpm)
Bottom Strip: Uterine Contractions
This line shows the mother’s contractions and allows you to assess:
- Frequency
- Intensity
- Duration
Parts of a Contraction
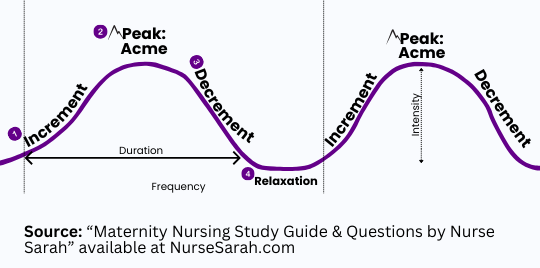
- Increment: Contraction building up
- Acme: Peak of the contraction
- Decrement: Contraction decreasing
- Relaxation: Resting phase between contractions
Types of Fetal Heart Rate Patterns
Accelerations: Temporary increase in fetal heart rate
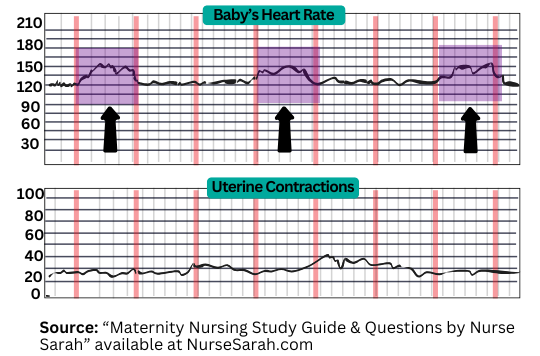
For a term fetus:
- Increase of ≥15 bpm above baseline
- Lasts at least 15 seconds
- Lasts less than 2 minutes
Causes:
- Fetal movement
- Contractions
What it Means?
- Baby is well-oxygenated
- Healthy neurologic response
Nurse’s Role:
- No intervention needed
- Continue monitoring and document
Early Decelerations
Key Concept: They mirror contractions
- Fetal heart rate dips when contraction starts
- Returns to baseline by the end of the contraction
- Heart rate remains within normal range (110–160 bpm)
Cause:
Head compression
- Contraction compresses fetal head
- Vagus nerve stimulation temporarily lowers heart rate
- Resolves as contraction ends
What It Means?
- Normal finding
- Common in active labor
Nurse’s Role:
- No intervention needed
- Continue monitoring and document
Variable Decelerations

Key Concept: Abrupt drops that look like a “V.”
- Sudden sharp drop in FHR
- May fall below 110 bpm
- Creates a V- or U-shaped pattern
- Can occur with or without contractions
Cause
Umbilical cord compression
- Cord = baby’s lifeline
- Compression decreases oxygen
- Causes sudden heart rate drop
What It Means?
- Not reassuring
- Requires intervention
Nurse’s Role:
- Change maternal position
- Side-lying, knee-to-chest, or Trendelenburg
- Administer oxygen (follow facility protocol)
- For fetal heart rate decelerations, recent evidence shows that routine high-flow oxygen is no longer recommended unless the mother is hypoxic. First-line interventions remain maternal repositioning, IV fluids, and stopping uterotonics.
- Stop Pitocin (if infusing)
- Perform vaginal exam: assess for cord prolapse
- Notify provider immediately
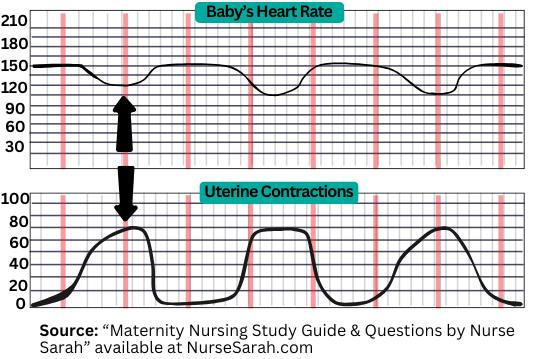
Late Decelerations
Key Concept: Occur after the peak of the contraction
- Heart rate drops after the contraction’s acme
- Does not recover until well after the contraction ends
Cause:
Uteroplacental insufficiency
- Placenta is not delivering adequate oxygen
- Indicates impaired fetal oxygenation
What It Means?
- Serious
- Requires immediate intervention
Nurse’s Role:
- Change maternal position to left lateral
- Administer oxygen (per facility protocol)
- For fetal heart rate decelerations, recent evidence shows that routine high-flow oxygen is no longer recommended unless the mother is hypoxic. First-line interventions remain maternal repositioning, IV fluids, and stopping uterotonics.
- Stop Pitocin
- Increase IV fluids (to improve placental perfusion)
- Notify provider immediately
- May require emergency C-section
You may be interested in Fetal Heart Monitoring Quiz
Maternity Nursing Study Guide

Save Time Studying and Actually Learn
Nurse Sarah’s Maternity Nursing Study Notes are designed to help you study faster, remember more, and stress less. With 151 pages of simplified summaries, illustrations, mnemonics, and visual breakdowns, you’ll breeze through even the trickiest OB topics.
Laser-Focused on What You’ll See on Exams
Whether you’re prepping for nursing school exams or the NCLEX®, these notes focus on the exact maternity/OB concepts you’re most likely to be tested on with no filler, no wasted time.
Memory Hacks, Visuals & Rationales That Make It Stick
Colorful illustrations and proven mnemonics help you actually retain the material, while 220 practice questions with in-depth rationales teach you the “why” behind the right answers so that you’re not just memorizing, you’re understanding.
Available at: NurseSarah.com and Amazon.com* (This is an affiliate link. We may earn a small commission if you make a purchase through this link at no extra cost to you).
References:
American College of Obstetricians and Gynecologists. (2025). ACOG clinical practice guideline No. 10: Intrapartum fetal heart rate monitoring: Interpretation and management. Obstetrics & Gynecology, 146(4), 583–599. https://doi.org/10.1097/AOG.0000000000006049
Anonymous says
I was really confused, searched multiple sites, The pictures and explanations here are amazing….THank you So Much, I Finally understand it!
OB Nursing Student, MI
S.L. Page says
Thank you so much 🙂 Glad it helped you out!
Stephanie Anderson says
Actually, studies show no decrease in infant mortality between FHM and intermittent auscultation with a Doppler, but they do show an increase in Caesarean births and other complications with FHM, due to the way it immobilizes a woman during labor and due to inaccurate readings. It is good to understand what the medical staff is reading on the monitor, but this technology does not save lives. Intermittent auscultation is supported by evidence, is what is used to know the baby’s heart rate during labor and delivery without electronic fetal heart monitoring, and it is still a relevant practice.
LISSETTE says
Thank you! I got it now. 🙂
S.L. Page says
Lissette,
So glad I could help you! Thanks for your kind words 🙂
S.L. Page
Candice says
you can always remember…
V C
E H
A O
L P
V= variable decels C= cord compression
E=early decels H= head compression
A= accels O= okay, not a problem!
L= late decels P= placental insufficiency
S.L. Page says
Candice,
Thank you so much for sharing this! VERY helpful and I’m sure other people will find it super helpful.
Sarah
Omo says
Thanks for your large heart. Good example of what this field is all about, blessing on you and your work.
S.L. Page says
Omo thank you so much for the comment 🙂 It feels good to get these comments. I appreciate it!
-Sarah
Anonymous says
oh my god..its so helpful,thanks alot…now m feeling confident about this topic
S.L. Page says
You’re very welcome =).