- Definition of myocardial infarction
- Anatomy of the coronary arteries
- Signs and Symptoms of MI
- Patho of myocardial infarction
- Causes of myocardial infarction
- How myocardial infarction is diagnosed
Lecture on Myocardial Infarction
Myocardial Infarction NCLEX Review
Definition: The heart’s myocardial tissue layer dies from decreased blood flow due to: Causes:- Blockage in the coronary artery from coronary artery disease (most common)
- Coronary spasms from illicit drug usage drugs like cocaine or hypertension. This causes constriction of the coronary artery and stops blood flowing to the heart muscle.
- Damage to the coronary artery due to coronary artery dissection. This is a tear in the inner layer “tunica intima” of the artery which causes blood to leak in the “tunica media”. This restricts the flow of blood through the coronary artery. It can happen spontaneously and occurs more likely in young, active women.
ECG/EKG Study Guide and Workbook for Nursing Students
You can get an eBook version here: “Nurse Sarah ECG Book” or a physical copy here: “ECG/EKG Interpretation Study Guide by Nurse Sarah“.
Pathophysiology of MI:
The coronary arteries supply the heart with nutrients. They branch off from the aorta into the left and right coronary artery. Left Coronary Arteries:
Important to note: Blockages in the left coronary arteries can cause the worst damage from a myocardial infarction. This is because blockages in the left coronary artery can cause anterior wall death which affects the left ventricle. Anterior MIs affect the most myocardial tissue, especially if the blockage occurs before it branches off and this can extend into the septum and lateral wall.
Left Coronary Arteries:
Important to note: Blockages in the left coronary arteries can cause the worst damage from a myocardial infarction. This is because blockages in the left coronary artery can cause anterior wall death which affects the left ventricle. Anterior MIs affect the most myocardial tissue, especially if the blockage occurs before it branches off and this can extend into the septum and lateral wall.
- Left anterior descending artery: supplies right and left ventricle and septum. This is the most common site for blockages.
- Left circumflex: supplies the left atrium and ventricle
- Right coronary artery: supplies the right atrium and ventricle
- Right marginal artery: supplies the right ventricle and septum
What happens to the heart muscle after an MI?
 When a coronary artery becomes 100% blocked the muscle cells die. Cell death is irreversible after about 30 minute. The cells are gone forever and can never be replaced.
When a coronary artery becomes 100% blocked the muscle cells die. Cell death is irreversible after about 30 minute. The cells are gone forever and can never be replaced.
- Early signs of an MI…no physical changes to heart muscle yet (until about 6-8 hours), but when the myocytes die cardiac enzymes are released: CK-MB (4 to 6 hours after MI), troponin (2-4 hours…most regarded) myoglobin (1 hours after injury…show injury but not too specific).
- Within 24-36 hours inflammation sets in and neutrophils come on the scene and congregate at the damaged tissue site. This causes complication of possible pericarditis. In addition, within 24 hours the heart fails to pump efficiently (cardiogenic shock) and arrhythmias can develop (atrial and ventricular dysrhythmia along with AV blocks).
- Within 10 days, granulation occurs when the macrophages come on the scene. They are WBCs who’ve came to clean up the dead cells and other components. However, the new tissue formed from granulation is not well formed and is weak. This increases the chance of cardiac rupture.
- Within 2 months scarring occurs, and the heart is affected in size and functionality due to increased collagen.
Signs & Symptoms of Myocardial Infarction
Remember the mnemonic: CRUSHING Chest pain (intense, heavy) Radiating chest pain that goes to left arm, jaw, back Unrelieved by nitroglycerin or rest (chest pain) Sweating (cold) Hard to breathe (shortness of breath) Increased heart rate, blood pressure or irregular heart rate Nausea with vomiting Going to be anxious and scared Note: Women can present differently by not having “heavy” chest pain. Their chest pain may be felt in the lower part of the chest, experience shortness of breath, and feel extremely fatigued. They may not seek immediate help because they think they are “just ill” with a sickness. Silent MIs: this is where the patient has no symptoms of chest pain. Mainly occurs in diabetics due to diabetic neuropathy where the nerves that feel pain are damaged in the heart.Diagnosing with Cardiac Markers & Other Tools
When the heart muscle is injured it releases cardiac markers overtime. This will help the health care provider know that something is going on along with a 12-lead EKG (and other tools). Blood Tests Cardiac markers:- Troponins: gold standard now used by most hospitals in assessing for an MI. It is a protein released from the heart when damage is present from a myocardial infarction. They are drawn in a series (troponin levels will elevate 2-4 after injury). They are usually drawn every 6 hours for 3 sets. The nurse’s role is to collect levels and monitor them for an upward trend. If levels are increasing, the physician will need to be notified.
- Myoglobin: an early cardiac marker released after heart injury (1 hour after injury). However, not very cardiac specific…used in early detection..will need more blood tests to further evaluate.
- CK: protein released when there is muscle damage (not specific to just the heart)…so CK-MB may be ordered to tell if it is the heart since CK-MB represents heart muscle (it elevates 4-6 hr after injury).
- Echocardiogram: ultrasound of the heart to look at the heart to see if there is damaged from an MI.
- Heart Cath: a procedure where a special dye is injected into the coronary arteries and an X-Ray is taken to see if there are any blockages, their locations, and if there is any muscle damage. If there is a blockage, the cardiologist will assess the need for stent placement or other techniques used to open the artery.
- Stress test with Myocardial Perfusion Imaging: assesses how the heart responses to stress and evaluate the blood flow to the myocardial muscle.
- EKG:
- Shows ischemia, injury, and infarction.
- Nurses role: obtaining EKG (or delegating it to be done) looking for any EKG changes and notifing md of them
- Compare newly obtained EKG to previous EKGs
 What are you looking for on the EKG? Please watch the lecture video above for an in depth explanation on this. This explanation starts at time mark: 18:33
What are you looking for on the EKG? Please watch the lecture video above for an in depth explanation on this. This explanation starts at time mark: 18:33
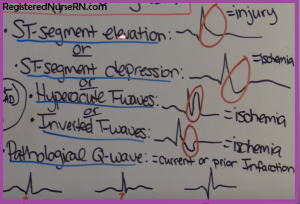
- ST-segment depression or elevation
- T-wave inversion or hyperacute
- Pathological Q-wave
- I, AVL, V5, V6: Lateral
- II, III, AVF: Inferior
- V 1, V2: Septal

- V 3, V4: Anterior
- “Heart Attack Signs & Symptoms | Cdc.Gov”. Cdc.gov. N.p., 2015. Web. 25 Sept. 2016.
- “How Is A Heart Attack Diagnosed? – NHLBI, NIH”. Nhlbi.nih.gov. N.p., 2015. Web. 26 Sept. 2016.