- Definition of coronary artery disease
- Anatomy of the coronary artery disease
- Patho of atherosclerosis
- Causes of coronary artery disease
- How coronary artery disease is diagnosed
Lecture on Coronary Artery Disease for NCLEX
NCLEX Review for CAD Part 1
Definition: the coronary arteries that deliver a constant supply of blood to the heart muscle begin to develop fatty plaques that can lead to restriction of blood flow to the heart. Fatty plaques are caused by a condition called ATHEROSCLEROSIS which creates fatty plaques in the artery walls.- Happens overtime
- Limits blood supply to the heart muscle and can rupture which can lead to thrombosis formation (hence causing a myocardial infarction)
- Atherosclerosis can also lead to hypertension, chest pain, and heart failure.
ECG/EKG Study Guide and Workbook for Nursing Students
You can get an eBook version here: “Nurse Sarah ECG Book” or a physical copy here: “ECG/EKG Interpretation Study Guide by Nurse Sarah“.
Main Arteries that feed the heart muscle:
 Left coronary artery which branches off to:
–Left circumflex artery: provides blood to left atrium & side and back of the left ventricle
–Left anterior descending artery: provides blood to the front and bottom of the left ventricle and front of the septum
Right coronary artery provides blood to the right atrium and ventricle and to the bottom part of the left ventricle and back of the septum and branches off to:
–Right marginal artery
-Posterior descending artery
These arteries can become atherosclerotic and factors that increase this include:
Left coronary artery which branches off to:
–Left circumflex artery: provides blood to left atrium & side and back of the left ventricle
–Left anterior descending artery: provides blood to the front and bottom of the left ventricle and front of the septum
Right coronary artery provides blood to the right atrium and ventricle and to the bottom part of the left ventricle and back of the septum and branches off to:
–Right marginal artery
-Posterior descending artery
These arteries can become atherosclerotic and factors that increase this include:
- Smoking
- Unhealthy: obese or overweight
- High cholesterol
- Sedentary lifestyle
- Diabetes
- Family history
Patho of Atherosclerosis Simplified:
 Blood flows through the artery which contains the red blood cells and lipids (LDL). LDL (low-density lipoproteins…the bad cholesterol) starts to adhere to the artery wall and grows overtime (risks factors can increase the rate at which it grows).
As it grows the patient is usually asymptomatic until the plaque becomes so big the artery starts to become narrow and blood flow to the heart becomes restricted. The patient can experience stable angina when the artery is blocked enough to slightly impede blood flow (however, blood is still able to get to the heart muscle), but the patient only has the chest pain during ACTIVITY. The activity increases the heart rate and puts strain on the heart which already has compromised blood flow, but when the activity STOPS the pain STOPS too.
****Collateral circulation can develop if chronic ischemia is experienced. This is where more than one artery forms to re-route blood to the heart muscle to make up for the decreased blood flow due to the blockage.
Patients with fatty plaque buildup in the arteries are at risk for the plaques to rupture. This can lead to coronary thrombosis where clotting material aggregates at the site of rupture and this leads to a significant or complete blockage of the coronary artery. Patients will have acute coronary syndrome with unstable angina or experience a myocardial infraction. This is a medical emergency.
Blood flows through the artery which contains the red blood cells and lipids (LDL). LDL (low-density lipoproteins…the bad cholesterol) starts to adhere to the artery wall and grows overtime (risks factors can increase the rate at which it grows).
As it grows the patient is usually asymptomatic until the plaque becomes so big the artery starts to become narrow and blood flow to the heart becomes restricted. The patient can experience stable angina when the artery is blocked enough to slightly impede blood flow (however, blood is still able to get to the heart muscle), but the patient only has the chest pain during ACTIVITY. The activity increases the heart rate and puts strain on the heart which already has compromised blood flow, but when the activity STOPS the pain STOPS too.
****Collateral circulation can develop if chronic ischemia is experienced. This is where more than one artery forms to re-route blood to the heart muscle to make up for the decreased blood flow due to the blockage.
Patients with fatty plaque buildup in the arteries are at risk for the plaques to rupture. This can lead to coronary thrombosis where clotting material aggregates at the site of rupture and this leads to a significant or complete blockage of the coronary artery. Patients will have acute coronary syndrome with unstable angina or experience a myocardial infraction. This is a medical emergency.
Signs and Symptoms of Coronary Artery Disease:
Many patients are asymptomatic during the early phases of CAD development.- Chest pain during activity (stable angina…not a medical emergency but patients need to let their doctor know about this chest pain so diagnostic testing can be performed). The pain may feel like heaviness on chest….can progress to unstable angina where the patient will have pain at rest and it is more intense…may not be relieved by Nitroglycerin.
- Shortness of breath: easily gets short of breath during activity because the blood supply is impeded to the heart muscle.
- Very tired, feeling run down especially with activity
Diagnosed with:
- Blood tests: Lipoprotein profile: total cholesterol, LDL, HDL, triglycerides
- EKG: assesses if there are any changes in the ST segments or t-waves (shows if there is a heart attack in the progress, previous heart attack, or compromised blood flow)
- A 24 or 48 hour Holter monitor may be ordered to watch the heart rhythm during the patient’s regular activities of daily living.
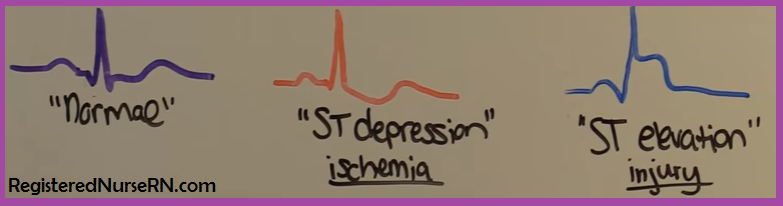
- ST segment depression: demonstrates ischemia that is reversible
- ST segment elevation: infarction where there is injury to the heart muscle
- During activity, if blood flow is reduced ST segment depression will occur and patient may have chest pain and then as activity stops the ST segment will return back to normal. A patient will probably then be ordered a heart cath to assess where the potential blockage is located.
- Also, a nuclear stress test may be ordered. This is where a tracer is injected and pictures of the heart are taken to assess blood flow of the heart muscle during activity.
- PCI (also called angioplasty): Percutaneous Coronary Intervention
- Balloon angioplasty: inflates a balloon in the blocked artery to compress the plaque against the artery wall and a stent is placed to allow blood to flow back through the artery.
- Atherectomy: removal of plaque from the artery
- “Anatomy Of The Heart – NHLBI, NIH”. Nhlbi.nih.gov. Web. 2 Sept. 2016.
- “Heart Health Tests: Medlineplus”. Medlineplus.gov. Web. 2 Sept. 2016.
- “What Causes Coronary Heart Disease? – NHLBI, NIH”. Nhlbi.nih.gov. Web. 3 Sept. 2016.