Coarctation of the aorta (CoA) review for nursing students!
In this review you will learn about the congenital heart defect known as coarctation of the aorta (CoA). This is a topic you will see on your pediatric nursing lecture exams and possibly the NCLEX exam.
After reviewing these notes, don’t forget to take the quiz that contains coarctation of the aorta NCLEX questions and to watch the lecture.
Lecture on Coarctation of the Aorta
Coarctation of the Aorta NCLEX Review
What is coarctation of the aorta? It’s a congenital heart defect where narrowing is present in a section of the aorta.
 Role of the Aorta
Role of the Aorta
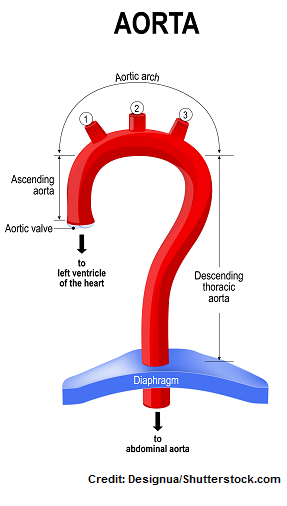
What does the aorta do? It’s the largest artery is the body! In addition, it’s a very important structure that comes off of the left ventricle that carries rich oxygenated blood to a collection of arteries (that branch off from the aorta) to supply the brain, upper/lower extremities, organs, and tissues.
There are various sections of the aorta that carry blood to very specific areas of the body:
Ascending aorta: branches off to supply the coronary arteries that feed the heart muscle.
Aortic arch: it branches off to supply the brain (hence the head and neck) and upper extremities.
Descending aorta: it branches off to supply the chest structures and ribs.
Abdominal aorta: found near the diaphragm and it branches off to supply the lower extremities and all the organs and tissues in the abdominal and pelvic cavity.
If there is any narrowing in the aorta, it is going to affect how blood is supplied to structures via the aorta.
In other words, in this condition, areas of the aorta that are found BEFORE the narrowing will experience a HIGH blood pressure, while areas found AFTER the narrowing will experience a LOW blood pressure (keep this concept in mind).
Quick Facts about Coarctation of the Aorta
- In CoA, the narrowing of the aorta tends to occurs AFTER the left subclavian artery, either before or after the ductus arteriosus.

- Types of CoA:
- Preductual (infantile type): narrowing between the subclavian artery and before the ductus arteriosus
- Postductal (adult type): narrowing occurs after the ductus arteriosus..most common in adults
- According to CDC.gov, 1,600 babies in the U.S. are born with this condition each year.
- It can be diagnosed during a prenatal visit with a fetal ultrasound or after birth with an echocardiogram.
- It’s thought to be caused by the tissue that makes up the ductus arteriosus, which has extended into a section of the aorta. So, when the ductus arteriosus NORMALLY after birth, a section of the aorta will narrow as well.
- Types of CoA:
Pathophysiology of Coarctation of the Aorta
The problem in this condition will be on the left side of the heart (hence the aorta). Remember the left side of the heart’s mission is to pump oxygenated blood that just LEFT the lungs to the body, and the aorta is the last structure in the heart that plays that vital role of delivering fresh oxygenated blood to the body.
When there is narrowing of a section of the aorta, the side that is proximal (before the narrowing)will have a high blood pressure, while the distal side (side after the narrowing) will have a lower blood pressure.
So, in other words, the branches of arteries that supply certain areas of the body found BEFORE the narrowing will experience a high blood pressure, while the branches of arteries that supply certain areas of the body found AFTER the narrowing will experience a decrease in blood pressure.
What are the structures that will experience high blood pressure BEFORE the narrowing?
Typically, it includes the heart (specifically the left ventricle…this can lead to heart failure overtime along with decreased cardiac output if not treated) because the left ventricle will have to work harder to pump against the high pressure. In addition, the upper body (includes head, neck, and upper extremities) is affected as well.
What are the structures that will experience decreased blood pressure AFTER the narrowing?
The lower body, particularly the pulses (femoral) and lower extremities (feel cool).
Therefore, an increase in blood flow to the upper body and decreased blood flow to the lower body will lead to:
Signs and Symptoms of Coarctation of the Aorta
**Signs and symptoms vary depending on the degree of narrowing….if severe: many babies will start to develop signs and symptoms suddenly (present with heart failure) shortly after birth when the bypasses from fetal circulation have closed, specifically the patent ductus arteriosus.
High pressure to the structures in the upper body and low pressure to the structures in the lower body will lead to:
- Nose bleeds
- Headaches (older children), babies very irritable
- Stroke
- Strong (bounding) pulse in the upper extremities
- Absent or very diminished pulses in femoral arteries/lower extremities (always want to check those on a newborn)
- Upper extremity blood pressure will be HIGHER than lower extremity (about 20 mmHg more when compared)….hence there will be hypertension in the upper extremities BUT not the lower
- Interscapular systolic murmur (auscultated on the left side of the back near the shoulder blades)
- Notching of the ribs due to collateral circulation (the body creates extra circulation to bypass the narrowing, which will be seen on the ribs and cause them to have a notched out appearance on a chest x-ray)
- Heart failure (decreased cardiac output with an enlarged left ventricle)
Nursing Interventions for Coarctation of the Aorta and Treatments
Monitoring for signs and symptoms of heart failure (decrease cardiac output or fluid volume overload): fluid in lungs with crackles, difficulty breathing, increased respiratory rate, fatigue, trouble feeding
Monitoring and reporting blood pressure and pulse differences in upper and lower extremities
Mild cases…may go undetected until later in childhood when abnormal blood pressures or pulses are detected in the upper vs. lower extremities…sometimes a heart murmur may be present (systolic) that is located on the back on the left side near the shoulder blades “interscapular”
If CoA is severe in a newborn, the patient may be started on a prostaglandin infusion to keep the ductus arteriosus open until surgery. This will help:
- decrease the work load on the left ventricle
- help blood to flow to the lower extremities
In addition, other medications may be ordered prior to surgery to help the heart’s function: Digoxin (causes the heart to pump stronger but at a slower rate) and diuretics (to remove fluid)
Surgery usually includes removing the area of the aorta that is narrow and reconnecting (anastomosis) the ends…usually done by 2 years old… may need balloon angioplasty later on to re-open the artery if narrowing occurs again, which is a complication that can happen later on.
Educating about treatments and possible complications:
- Aorta can narrow again at some point and will require a procedure to re-open
- Hypertension: some child can continue to experience hypertension long-term and will need medications to control
- Long-term follow-up care with a cardiologist
References: