This is a large group of beta-lactam antibiotics used to target a variety of gram-positive and gram-negative bacteria. There are five generations of Cephalosporins currently.
These antibiotics are similar to another group of beta-lactam antibiotics called the Pencillins. Their similarity arises from their chemical structures because both types are made up of a beta-lactam ring.
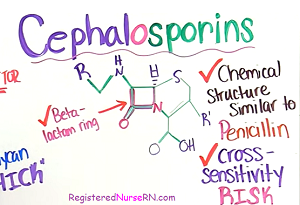
Due to this, there is a cross-sensitivity risk, which means if a patient is allergic to Pencilins they may also be allergic to Cephalosporins, especially the older generations of Cephalosporins.
Don’t forget to watch the Cephalosporin lecture and to take the free quiz with Cephalosporin NCLEX style questions.
What medications are Cephalosporins and what do they target?
Cephalosporins are fairly easily to recognize on a patient’s medication list because most of the generic names start with a Ce and has Cef or Cephal at the beginning, which is helpful.
Cephalosporins can be divided into five generations. The earlier the generation the more narrow the reach of the antibiotic. While newer generations have a broader reach and can take on some serious bacterial infections.
Let’s look at them (a few medication names are listed with each generation…this is not a complete list):

First Generation: mainly target gram-positive cocci like Staphylococci and Streptococci and some gram-negative like Klebsiella pneumoniae and E.coli.
- Cefazolin
- Cephalexin
Second Generation: targets include first generation, but expands to cover more gram-negative (Haemophilus influenza and Neisseria gonorrhaeae). It can also target gram-negative anaerobes, especially the last two on this list (Cefoxitin and Cefotetan) like *Bacteroides fragilis.
- Cefaclor
- Cefuroxime
- Cefoxitin*
- Cefotetan*
Third Generation: targets even more gram-negative bacteria (like Proteus) and some gram-positive but not as much reach as the first and second generation in respect to gram-positive.
- Cefotaxime
- Ceftriaxone (remember: don’t administer with calcium solutions because it can cause calcium precipitation)
- Ceftazidime: only one in this group that can target Pseudomonas aeruginosa
Fourth Generation: wide target of both gram-negative and positive and even better coverage for Pseudomonal infections.
- Cefepime
Fifth Generation: targets gram-negative and gram-positive and is the only Cephalosporin generation that can take on MRSA
- Ceftaroline
How are they administered?
Parenteral (IV or IM) and some are orally
How do Cephalosporins work?
Goal: Inhibit cell wall synthesis by having an overall bactericidal affect meaning it kills the bacteria
How does it do this?
Cephalosporins target a specific part of the cell wall known as peptidoglycan, which is a layer that makes up a significant portion of the bacteria’s cell wall.

The thickness of the layer varies depending on if we’re talking about a gram-positive or gram-negative bacterium. For example, gram-positive bacteria have a thick layer of peptidoglycan, whereas gram-negative have a thinner layer.
Regardless of its thickness, peptidoglycan’s job is to provide a strong, firm, protective layer for the cell wall and plays a role in properly handling the intense osmotic pressure that occurs within the cell.
Therefore, if the peptidoglycan layer is manipulated in how it synthesizes (specifically how parts of it cross-links together), the cell wall will lose its strong protective layer and the osmotic pressure will be too intense for the cell causing it to rupture and die. Fortunately, this is exactly what we want to happen.
So, let’s simplify how the peptidoglycan layer forms and how Cephalosporins affect it’s synthesis:
Peptidoglycan is a polymer made up of a network of polysaccharide strands (hence sugars) and amino acids. These strands consist of N-acetylglucosamine (NAG) and N-acetylmuramic acid (NAM), which stack beside each other.
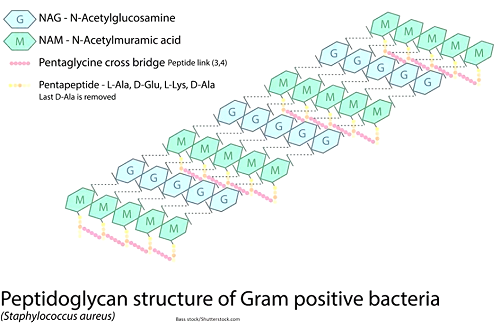
Now coming off the N-acetylmuramic acid (NAM) are several amino acids which help cross-link (hence connect) these stacks of strands so there is a tight, firm bond.
To help this cross-linking process happen, Penicillin-Binding Proteins (PBPs) such as transpeptidase enzymes and other types will make this process happen.
Now, it’s important to note that if this cross-linking can’t occur the peptidoglycan layer loses its ability to function and the cell will rupture because it can’t withstand the intense osmotic pressure within the cell. So, crossing-link properly is essential for peptidoglycan synthesis.
Therefore, that is the process beta-lactam antibiotics (like Cephalosporin) target. Remember from earlier, I talked about a beta-lactam ring within their chemical structure. Well this beta-lactam ring binds to these Penicillin-Binding Proteins. When binding to these proteins occurs it inhibits successful cross-linking, which leads to a faulty peptidoglycan layer and inhibits cell wall synthesis. In turn, the bacterium’s cell ruptures and dies!

Nursing Considerations for Cephalosporins?
- Before administration always assess allergies
- Remember to ask for a Penicillin allergy and if patient has one, ask about what type of reaction they had and report it to the physician for further orders
- Monitor for effectiveness (is it working?)
- Obtain any cultures, if ordered
- Monitor for adverse reactions and provide patient education
To help us remember these important concepts let’s remember:
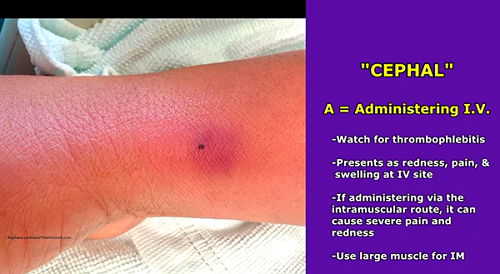
“Cephal” from the word Cephalosporin
Creatinine and BUN labs need to be monitored…it can be nephrotoxic
- Cephalosporins can be toxic to the kidneys, especially high doses and if the patient has some renal insufficiency.
- Nurses roles is to monitor intake and output (urinary output in adults 30 mL/hr) and lab levels.
ETOH intolerance (known as disulfiram –like reaction)…educate NO alcohol while taking
- Disulfiram is a medication prescribed to treat alcohol addiction (trade name is called Antabuse). It causes a person to become intolerant to alcohol after they drink it. Unfortunately, if a patient drinks alcohol or takes medications with alcohol in it, it can lead to signs and symptoms of alcohol intolerance if they are taking certain Cephalosporins.
- Educate the patient this can happen up to 3 days after the last dose of the antibiotic.
- Reaction presents with: vomiting, nausea, flushing, sweating, headache, dizziness etc.
Pseudomembranous colitis: major inflammation of the large intestine affected by a C. diff infection (antibiotic-associated colitis)
- Fluoroquinolones can also cause this along with other antibiotics when used in high dosages for long periods of time.
- Nurse: monitor stool pattern, temperature, and white blood count
- This condition can present with severe watery stool, fever, abdominal cramps, and elevated white blood count (leukocytosis)
- Collect stool for c.diff test per physician’s order
- NOTE: sometimes Cephalosporin can cause GI upset which can present with vomiting, diarrhea, and nausea. Sometimes administering oral forms of this antibiotic with food may help decrease this.
Hypersensitivity reaction: (assess for history of penicillin allergy)
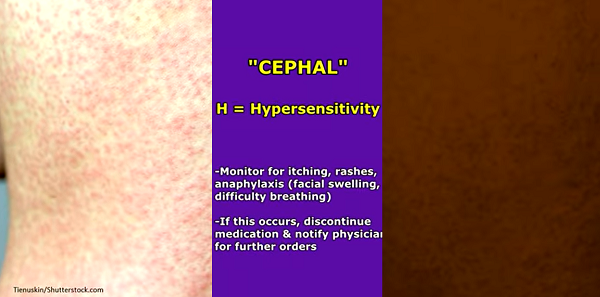
- Monitor for: intense itching, skin rashes that are very red and noticeable, and in worst cases anaphylaxis with facial swelling and dyspnea
- Discontinue and notify physician for further orders
Administering IV watch for thrombophlebitis (redness, pain, and swelling at IV site) and Intramuscular injection can cause pain and redness at the site….use a large muscle for IM administration.
Lowers prothrombin (hypoprothrombinemia) which increases risk for bleeding because it affects vitamin-K’s role in clotting which helps with the creation of prothrombin…monitor for PT/INR levels and for bleeding or bruising
Test your knowledge on this material with this Cephalosporin Quiz.
References:
GlaxoSmithKline. (2004). ANCEF ® cefazolin for injection. Retrieved from https://www.accessdata.fda.gov/drugsatfda_docs/label/2004/50461slr139_ancef_lbl.pdf
Bui T, Preuss CV. Cephalosporins. [Updated 2022 Nov 6]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK551517/
Popham DL, Young KD. Role of penicillin-binding proteins in bacterial cell morphogenesis. Curr Opin Microbiol. 2003 Dec;6(6):594-9. doi: 10.1016/j.mib.2003.10.002. PMID: 14662355.