This NCLEX review will discuss ARDS (acute respiratory distress syndrome).
As a nursing student, you must be familiar with ARDS and how it affects patients. In addition to the signs and symptoms, nursing interventions, and treatments for this condition.
Don’t forget to take the free quiz that contains ARDS nclex questions after reviewing this material.
ARDS NCLEX Lecture
ARDS NCLEX Review
What is ARDS (acute respiratory distress syndrome)? It’s a type of respiratory failure that occurs when the capillary membrane that surrounds the alveoli sac becomes damaged, which causes fluid to leak into the alveoli sac.
Result? Impaired gas exchange! Gas exchange doesn’t occur properly due to many reasons, such as: fluid in the alveoli sac, collapsed alveoli sacs, and a decrease in lung compliance (hence the lungs are becoming less elastic….”stiff”).
This will lead to oxygen not being able to cross the alveolar capillary membrane to go back in the blood to oxygenate it, which will result in hypoxemia. In turn, the organs of the body will suffer due to this and death can occur if treatment does not happen. In majority cases of ARDS, the patient will need respiratory assistance via a ventilator with PEEP (discussed in detail below).
Nurse Sarah’s Notes and Merch
Just released is “ABG Interpretation Notes, Mnemonics, and Workbook by Nurse Sarah“. These notes contain 64 pages of Nurse Sarah’s illustrated, fun notes with mnemonics, and worksheets that include over 90 ABG practice problems and 60 test review questions covering ABG concepts.
You can get an eBook version here or a physical copy of the book here.
Quick Facts about Acute Respiratory Distress Syndrome (ARDS)
- It has a fast onset!
- It tends to occur in people who are already sick (hospitalized) and develops as a complication. For example, a patient who has experienced severe burns is at risk for ARDS due to the systemic inflammation present in the body.
- ARDS has a high mortality rate!
What can cause the capillary membrane to become more permeable and leak fluid? Usually events that lead to major systemic inflammation in the body, which can be indirectly damage the capillary membrane or directly damage the capillary membrane.
Indirect vs. Direct Injury to the Capillary Membrane
Indirect (source isn’t the lungs): the capillary membrane is INDIRECTLY damaged. There is a systemic inflammatory response system (SIRS) by the immune system.
Common Causes:
- *Sepsis (most common and there is a very poor prognosis if the patient has a gram-negative bacteria)
- Burns
- Blood transfusion (multiple)
- Inflammation of the pancreas (pancreatitis)
- Drug overdose
Direct (source is the lungs)….capillary membrane is DIRECTLY damaged
- Pneumonia
- Aspiration
- Inhaling a toxic substance
- Significant drowning event
- Embolism
How it happens? Pathophysiology: Phases (varies on severity…this is worst case scenario)
Exudative Phase: occurs about 24 hours after injury to the lung (directly or indirectly)
What happens during this phase?
- Damage to the capillary membrane that leads to pulmonary edema. This causes the leaking of fluid, proteins, and other substances into the interstitium and then into the alveoli sac. It is very important to note this fluid contains a LOT of protein. Significance? Remember proteins regulate water pressure, oncotic pressure! So, if the fluid is high in protein it’s going to draw even MORE fluid into the interstitium and then the alveoli sac.
- Cells that produce surfactant become overwhelmed and damaged.
- Role of surfactant: decreases surface tension in the lungs. In other words, the alveoli sacs stay stable. Therefore, when a person exhales the sac does NOT collapse.
- A decrease in surfactant creates an unpredictable alveoli sac that can easily collapse. This leads to:
- ATELETASIS will occur (collapse of the lung tissue)
- To make matters worse: a membrane that is made up of dead cells and other substances start to collect on the alveoli. This is called a hyaline membrane. This membrane will continue to develop in the next phase and will cause the lungs to become LESS elastic and can further impair gas exchange!
- A decrease in surfactant creates an unpredictable alveoli sac that can easily collapse. This leads to:
- Role of surfactant: decreases surface tension in the lungs. In other words, the alveoli sacs stay stable. Therefore, when a person exhales the sac does NOT collapse.
End Result? With all the fluid in the alveoli sac (pulmonary edema), development of a hyaline membrane, collapsing of the sacs, decreased surfactant = inadequate ventilation where alveoli sacs are NOT getting enough air (leading to V/Q mismatch) AND a hallmark sign and symptom: REFRACTORY HYPOXEMIA
Refractory hypoxemia is where the patient will maintain a low blood oxygen level even though they are receiving high amounts of oxygen!
Early: Due to all this the patient will experience an increase in breathing (still have hypoxemia). WHY? The body is trying to increase the oxygen level, but it won’t be able to! This will cause the patient to blow off too much carbon dioxide (CO2 can still cross the membrane but O2 can’t)….respiratory ALKALOSIS will develop BUT in the late phase (as the patient progresses to the 2nd and 3rd phases (late), carbon dioxide levels start to rise. This is because the hyaline membrane continues to develop leading to carbon dioxide not being able to cross over to be exhaled, and the patient will no longer be able to maintain breathing due to weak respiratory muscles. Respiratory acidosis will start to develop later on.
Proliferative Phase: occurs about 14 days after the injury (grow or reproduce new cells quickly)
- repair structures, fluid in the sac is reabsorbed, but lung tissue becomes very dense and fibrous….lung compliance and hypoxemia becomes even worse
Fibrotic Phase: occurs about 3 weeks after injury….major fibrosis of the lung tissue, decreases lung compliance and hypoxemia with dead space filling the lungs.
Patients who enter the fibrotic phase will have major lung damage and poor recovery.
Pathophysiology of ARDS in a Nutshell
Atelectasis (alveolar sac fill with fluid and collapse…pulmonary edeam)
Refractory Hypoxemia
Decrease in lung compliance (lung aren’t as elastic or stretchable….hyaline membrane develops)
Surfactant cell damaged (decrease in surfactant production)
Signs and Symptoms of ARDS
In the very early phase: sign and symptoms are hard to detect. At first the fluid is leaking in the interstitum so lung sounds may be normal or random a crackle here or there. But as it progresses the patient will have difficulty breathing and be “air hunger”. There will be an increased respiratory rate, low oxygen in the blood and respiratory alkalosis.
Then as time goes on:
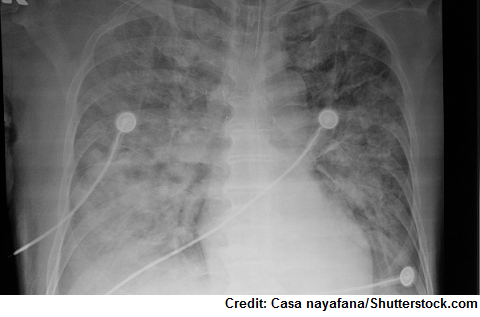
- Symptoms of full respiratory failure: tachypnea, difficulty breathing, major hypoxemia even though receiving a high about of oxygen (refractory hypoxemia), cyanosis, low oxygen saturation, mental status change (tired, confused), tachycardia, chest retractions, decrease lung compliance, lung sound: crackles throughout, low Pao2, high PaCo2 x-ray with white-out of bilateral lung infiltrates
Nursing Interventions for ARDS (acute respiratory distress syndrome)
Maintain airway/respiratory function:
Most patients with ARDS will need: mechanical ventilation with PEEP (positive end-expiratory pressure)
- The patient will need high amounts of PEEP because of the collapsed sacs, stiffening of the lung, and pulmonary edema. Usually the pressure is anywhere from 10 to 20 cm of water. This high amount of pressure will open the sacs, improve gas exchange, and help keep them clear of fluid.
- Nurse: high PEEP can cause issues with intrathoracic pressure and decrease cardiac output (watch out for a low blood pressure) along with hyperinflation of the lungs (possible pneumothorax or subq emphysema…this is where air escapes into skin from a lung leaking air)
Monitoring ABGs
Positioning to help with respiratory function:
Prone Positioning: turning the patient from supine to prone (putting the patient on their belly)
- This helps improve oxygen levels without actually giving the patient a high concentration of oxygen! Remember in this position the heart will shift forward and not compress the back of the lungs and it will help drain areas of the lungs that normally can’t be drained in the supine position. So, this will:
- Help with perfusion and ventilation (helping with correcting the V/Q mismatch)
- Help move secretions from other areas that were fluid filled and couldn’t move in the supine position
- Help improve atelectasis.
How does the MD know if this is pulmonary edema caused by a cardiac issue like heart failure or due to a leaking capillary membrane? A pulmonary artery wedge pressure can help with that!
- This is where a pulmonary catheter with a balloon is inserted into the pulmonary arterial branch
- If the reading is less than 18 mmHg it indicates ARDS, but if it’s greater than this number it indicates a cardiac problem.
Assessing other systems of the body to make sure they are getting enough oxygen: mental status, urine output, heart (blood pressure and cardiac output with PEEP)
Preventing complications: pressure injury, blood clots, infection related to ventilator, nutrition, pneumothorax
Administering drugs: corticosteroids (help with inflammation), antibiotics (preventing and treating infection), fluids colloids or crystalloids solutions if cardiac output decreased along with drugs like that have an inotropic effect (helps with heart muscle contraction), GI drugs for stress ulcers
References:
ARDS | National Heart, Lung, and Blood Institute (NHLBI). Retrieved from https://www.nhlbi.nih.gov/health-topics/ards
Acute respiratory distress syndrome | Genetic and Rare Diseases Information Center (GARD) – an NCATS Program. Retrieved from https://rarediseases.info.nih.gov/diseases/5698/acute-respiratory-distress-syndrome