Deep Vein Thrombosis (DVT) NCLEX review for nursing students!
A deep vein thrombosis is a type of venous thromboembolism (VTE). It is important that you’re familiar with the signs and symptoms, preventive measures, treatment, and pathophysiology for a DVT.
Lecture on Deep Vein Thrombosis (DVT)
Deep Vein Thrombosis (DVT) NCLEX Review
What is it? It’s the formation of a clot within a deep vein.
- It’s a type of venous thromboembolism (VTE), which is a blood clot that starts in the vein. The other type of VTE is a pulmonary embolism, which is where a deep vein thrombosis breaks off within the vein and goes to the lungs.
- A pulmonary embolism is a risk from the development of a DVT.
What veins are most susceptible for a DVT?
Veins located in the pelvis, lower leg (calf), and thighs. This includes: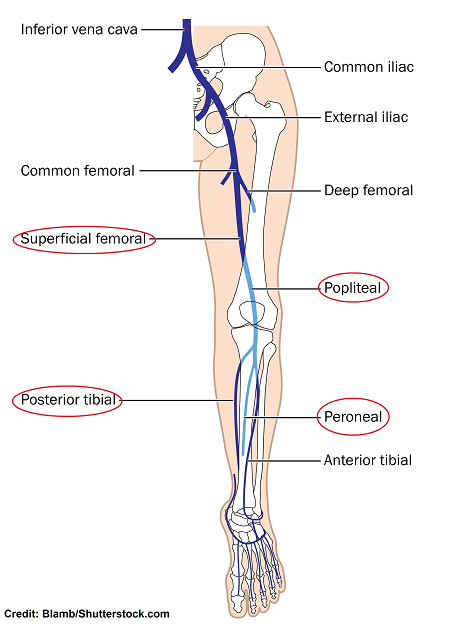
- Peroneal and posterior tibial in the calves (found in the lower leg)
- Popliteal and superficial femoral (found in the thighs)
DVTs tend to occur in the lower extremities (legs), but can occur in the upper extremities as well. However, DVTs in the lower extremities tend to have a higher chance of breaking off and turning into a PE (pulmonary embolism).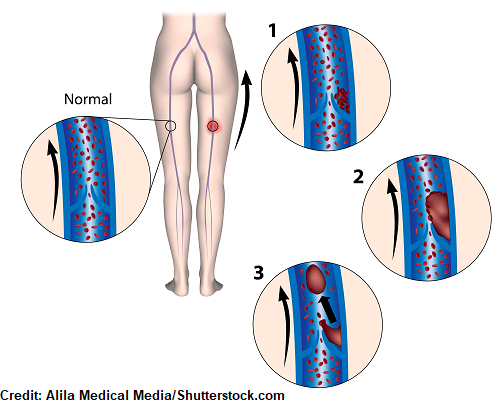
What factors play a role in the development of a DVT? To answer that question, we must review Virchow’s Triad.
Virchow’s Triad gives us three main factors that can lead to blood clot formation within a vein. Remember there are THREE factors (hence why it’s called a Triad).
Anyone can develop a deep vein thrombosis, especially if these risk factors are present.
Remember: “SHE”
Stasis of Venous Circulation:
Blood cannot just hang out and become static within a vessel. If it does this the blood will start to clump up (due to the present of platelets) and form a clot. The venous system is responsible for taking deoxygenated blood BACK to the heart. Therefore, the blood has to flow back to the heart via the veins, and it does this with the assistance of healthy vein valves and the muscles within the extremity. If the vein’s valves are damaged or the muscles aren’t working (or being used) blood isn’t going to flow back very well and a blood clot can develop.
What are some conditions that cause stasis of blood flow?
- Immobilized
- Varicose Veins
- Surgery (hip or knee)
- Traveling for long hours without moving extremities
- Obstruction: late pregnancy, obesity
- Heart failure (left ventricular dysfunction)
- Atrial fibrillation
Hypercoagulability: let the name of this factor help you…hyper means increase or high and coagul refers to the coagulation process in the body (hence forming a clot). Therefore, the patient has a high risk of forming a blood clot. The main reason for this is due to a disease process, but it can be due to other reasons. NOTE: This list is not a complete list.
What are some conditions that cause an increased risk of forming a clot within the vessel?
- Cancer
- Severe illness (sepsis)
- Dehydration
- Usage of Estrogen (birth control)
- Heparin Induced Thrombocytopenia (HIT)
- Postpartum Period
Endothelial damage to the vein: This endothelial is a layer of cells that lines the inside of the vein. Damage to this layer can be from a direct or indirect cause, but regardless it stimulates platelets and the coagulation process. So think of anything that damages the lining inside the vessel.
What are some conditions that cause damage the endothelial lining?
- IV drug usage ( also venipuncture…drawing blood from a vein)
- Indwelling devices (central line catheter, IV line, or heart valves etc.)
- Medications that are damaging to the vein
- Trauma or injury to the vessel (surgery)
How does a clot form and what substances are involved?
Regardless of the factor(s) contributing to the blood clot, as identified by Virchow’s Triad, platelets are involved. The platelets start to collect at the edges of the vessel, usually within the cusps of the vein’s valve. Platelets normally help create a seal to stop the bleeding. So, when they start to work within the vessel it recruits other chemicals called clotting factors.
Clotting factors cause fibrin to be created. Fibrin causes the big problem in terms of a clot developing because fibrin is like strands of mesh. This causes WBCs, RBCs, and platelets to stick together within the vein. This forms a clot and it continues to grow, which can eventually break off and enter venous circulation.
So we’ve seen how a clot forms now let’s talk about what you can see in your patient that may have a DVT.
Signs and Symptoms of a Deep Vein Thrombosis
- Redness
- Swelling
- Very warm
- Pain
- Homan’s Sign: NOT reliable for detecting a DVT because of false positives… but know for exams how to elicit a response:
- Extend the patient’s leg and manually dorsiflex the patient’s foot (bend it up towards the shin). If it causes the patient pain, it considered a Positive Homan’s Sign.

- Extend the patient’s leg and manually dorsiflex the patient’s foot (bend it up towards the shin). If it causes the patient pain, it considered a Positive Homan’s Sign.
Nursing Interventions for DVT (Deep Vein Thrombosis)
- Can be diagnosed with an ultrasound.
- D-dimer (also called fibrin degradation fragment)
- This is a blood test that assesses for fibrin degradation fragment (d-dimer), it’s a fibrin degradation product.
- Used to diagnose blood clots or Disseminated Intravascular Coagulation (DIC).
- This is a protein fragment that hangs out in the blood when a clot breaks down. So this means a clot has formed and has started to break down.
- A D-dimer doesn’t tell us where the clot is located, so it will need to be further investigated by the MD. Also, a positive result doesn’t necessarily mean the patient has a clot because some disease processes can cause a false positive.
- Example: Liver disease, MI, surgery (heart), cancer, pregnancy
- Normal d-dimer?
- D-dimer can be reported in fibrinogen equivalent units (FEU) or d-dimer units (DDU).
- Normal level: <500 ng/mL FEU or <250 ng/mL DDU
Prevention…very simple but so beneficial…nurses play a HUGE role with this!
Assess for the signs and symptoms and risk factors above and take precautions with prevention.
Application and regular usage of pneumatic compression devices like (SCDs) Sequential Compression Device per MD order. These devices wrap around the legs and inflate and deflate to help move blood flow (similar to walking).
- They must fit properly.
- They’re NOT to be applied to the extremity that has an active DVT (can lead to dislodgement).
- Make sure the patient is wearing them while sitting or in bed. Take them off when the patient is walking. Make sure they’re plugged in, actually inflating and deflating (ask the patient). These devices can come unplugged from wall and quit working. Also, make sure they are changed and cleaned regularly (they can become sweaty and smelly).
Patient needs to be ambulating daily and out of the bed with all meals, if possible.
Teach patient to perform exercises by flexing and extending feet and legs every hour while awake.
Compression stockings per MD order: provides a specific amount of compression to help decrease risk of blood clot development.
Prophylactic medications: after surgery (post-op), especially joint replacement surgery like the hip… Example: Enoxaparin (subq injection)
If patient has a DVT:
“Deep Clot”
Don’t rub or massage affected extremity (can dislodge clot)
Elevate the affected extremity above heart level (promotes blood return and decreases swelling)
Ensure bed rest
Pharmacological Measures Include:
- Anticoagulants: do NOT break up the clot but helps prevent new ones from developing and from getting bigger.
- Heparin: Indirect thrombin inhibitor
- Enhances the activity of antithrombin III, which will inhibit thrombin and the conversion of fibrinogen to fibrin. (acts fast) given IV or subq…weight-based
- Monitor aPTT (activated partial thromboplastin time): 1.5 to 2.5 times normal ranges
- >80 seconds risk for bleeding….dose decreased
- <60 seconds NOT therapeutic…risk for clots and may need dosage increased
- Used in combination with Warfarin until INR is therapeutic and then Heparin is discontinued.
- Antidote: protamine sulfate
- Warfarin: Vitamin K antagonist
- Since it’s a Vitamin K antagonist, it will work to inhibit clotting factors from using Vitamin K.
- Slow onset….takes 3-5 day for patient to become therapeutic
- Taken orally
- Monitor PT/INR…therapeutic INR is 2-3 (less than 2…not therapeutic) and greater than 3 at risk for bleeding)
- Antidote: vitamin K
- Thrombolytics: catheter-directed thrombolysis with tPA…clot busting agent delivered directly to the clot (watch out for bleeding).
- Filter: IVC filter (small metal device placed in the inferior vena cava to prevent blood clots from enter the heart and lungs)
- Many times this is placed for patient who can’t take anticoagulants.

- Many times this is placed for patient who can’t take anticoagulants.
- Heparin: Indirect thrombin inhibitor
Compresses (warm/moist) helps pain and circulation
Leg circumference measurement (calf)…measure about 10 cm or 4 inches below tibial tuberosity…watch out for a 3 cm circumference or more measurement when compared to the non-affected calf.
Observe for signs and symptoms for PE
- sudden shortness of breath, decreased oxygen saturation, fast heart rate, chest pain, very anxious, sweating, coughing
Tight compression stockings (thigh or knee high compression) per MD order…helps promote blood flow and decreases swelling (change regularly and show patient how to apply)
- Fitted and applied properly as prescribed
- Compression stockings may prevent PTS (post-thrombotic syndrome), which happens sometimes after the development of a DVT. This is because vein valves and walls became damaged due to the clot…blood doesn’t flow in the right directions (back to the heart).
Now test your knowledge by taking the Deep Vein Thrombosis NCLEX Questions quiz.
References:
Diagnosis and Treatment of Venous Thromboembolism | CDC. (2019). Retrieved 1 November 2019, from https://www.cdc.gov/ncbddd/dvt/diagnosis-treatment.html
Venous Thromboembolism | National Heart, Lung, and Blood Institute (NHLBI). Retrieved 1 November 2019, from https://www.nhlbi.nih.gov/health-topics/venous-thromboembolism
What is Venous Thromboembolism? | CDC. Retrieved 1 November 2019, from https://www.cdc.gov/ncbddd/dvt/facts.html