Autonomic Dysreflexia (hyperreflexia) NCLEX review for nursing students!
Autonomic dysreflexia (AD) occurs in patients who have experienced a spinal cord injury, and it’s most likely to common in patients who have suffered a T6 or higher injury. This condition happens when an irritating stimulus occurs below the site of spinal injury, which leads to an exaggerated sympathetic nervous system reflex.
As the nurse, it is very important to know how to detect, prevent, and act when a patient experiences AD. This review is part of a neuro review, so be sure to check out those other NCLEX reviews.
Don’t forget to take the quiz that contains Autonomic Dysreflexia NCLEX Questions.
Lecture on Autonomic Dysreflexia
Autonomic Dysreflexia (Hyperreflexia) Nursing Review
What is it?
Let’s break down the word of this condition to help us with that:
Hyper= excessive or exaggerated
Reflex = reflex response of some type
Autonomic = involuntary nervous system that controls functions we can’t do consciously
When you put all that together, it means that autonomic hyperreflexia (dysreflexia) is an exaggerated (excessive) reflex response by the autonomic system (specifically the sympathetic nervous system).
This reflex response by the sympathetic nervous system will be unopposed by the parasympathetic nervous system, which makes it dangerous.
What causes this exaggerated reflex response?
 It occurs due to an irritating (potentially harmful) stimulus below the site of injury in patients who have a spinal cord injury, and it results in severe hypertension.
It occurs due to an irritating (potentially harmful) stimulus below the site of injury in patients who have a spinal cord injury, and it results in severe hypertension.
It’s a medical emergency that must be PREVENTED and quickly DETECTED. It can lead to a stroke or seizure and be fatal.
Who’s at HIGH risk for developing Autonomic Dysreflexia?
A patient who has experienced a T6 or higher spinal cord injury.
What are the main BIG causes of Autonomic Dysreflexia?
Anything that is an irritating stimulus that occurs BELOW the site of the spinal cord injury can lead to it, BUT there are 3 big causes you need to remember.
Remember the 3 Big B’s….
- Bladder issue: example would be a distended or urinary tract infection
- Bowel issue: like hard stool that collects in the rectum leading to impaction
- Break down of skin: due to any type of binding devices or clothing, pressure injury, burns, infection, cuts etc.
Miscellaneous causes: birthing process, sexual intercourse, menstruation, or anything procedure that causes stimulation below the site of injury
Pathophysiology of Autonomic Dysreflexia
First, we need to review the autonomic nervous system:
The autonomic nervous system controls the involuntary functions of the body, and it’s divided into two branches. These two branches (sympathetic and parasympathetic) work to balance each out by opposing each other and this helps maintain homeostasis in our body. If one of these systems is stimulated and unopposed (meaning the other system that normally opposes it does nothing to reverse the reaction), it could result in major problems.
Sympathetic and Parasympathetic Nervous System
 Sympathetic Nervous System is the “fight or flight system” that saves our life when something bad occurs. If something is wrong in the body or it perceives danger, it causes the body to react to it…hence to an irritating, potentially harmful stimulus.
Sympathetic Nervous System is the “fight or flight system” that saves our life when something bad occurs. If something is wrong in the body or it perceives danger, it causes the body to react to it…hence to an irritating, potentially harmful stimulus.
Some functions of this system include:
- Constriction of vessels (increases blood pressure)
- Stimulates sweat glands
- Increases blood flow to skeletal muscle for potential activity to react to dangerous stimulus
- Increases blood glucose for energy
- Bronchodilation to help you breathe better so you can run and get out of danger
- Increases heart rate
- Dilates pupils for better vision
Parasympathetic Nervous System is the “rest and digest system” that helps us chill, relax, eat, and reproduce. It helps calm down the sympathetic nervous system when it is activated.
Some functions of this system include:
- Dilation of vessels (to decrease blood pressure)
- Slows down heart through vagal nerve stimulation
- Salivation
- Bronchoconstriction
- Constrictions pupils
Therefore, these two systems work together, and if one kicks into play the other will help try to balance it out to maintain homeostasis.
To do this properly and successfully, it must have a healthy and intact spinal cord to send the messages/impulses back and forth. If the spinal cord is injured the autonomic nervous system won’t be able to properly communicate with the brain and the person won’t know there is a problem that is occurring below the site of injury.
So, let’s talk about what’s occurring in autonomic dysrflexia when an irritating stimulus is presenting below the site of spinal injury…
-
- An irritating stimulus is presenting BELOW the site of injury…remember one of the Big B’s above.
- Nerves send impulses away from the stimulus that something is wrong in hopes of letting the brain (hence the patient) to do something about it, but this is unsuccessful because the injury has BLOCKED the transmission of signals.
- However, remember the autonomic nervous system is still in intact but doesn’t communicate like normal. So, the irritating stimulus causes an EXAGGERATED reflex by the sympathetic nervous system.
- This leads to vasoconstriction (narrowing of vessels) below the site of injury, which will cause hypertension.
- The baroreceptors in the carotid sinus and aorta sense this extreme high blood pressure and attempt to do something about it by stimulating the parasympathetic nervous system. Normally, this would help balance out the affects created by the sympathetic system if the impulses could travel pass the site of spinal injury, but they can’t…remember their blocked. Therefore, parasympathetic compensatory affects only occur really above the site of injury.
-
- Parasympathetic activity causes above the site of injury:
- Vagal nerve stimulation occurs and it drops the heart rate in hopes of decreasing the blood pressure (but it doesn’t work)…instead the patient can become bradycardic.
- Vasodilation occurs ABOVE the site of injury but not below the site of injury. This causes flushing above the site of injury. Remember normally vasodilation would help lower the blood pressure but because of the spinal injury the vasodilation can occur only above the site of injury and vasoconstriction is still occurring below the site of injury.
- Parasympathetic activity causes above the site of injury:
6. These compensatory mechanisms by the body are not effective in lowering the blood pressure because vasoconstriction is still occurring below the site of injury.
-
7. Irritating stimulus needs to be removed so this reflex response will stop.
Signs and Symptoms of Autonomic Dysreflexia
- Throbbing Headache
- Hypertension: normal blood pressure for a patient with a T6 or higher spinal cord injury is usually a systolic 90-110 mmHg….watch for systolic 20-40 mmHg higher than their baseline because this is worrisome
- Flushing of skin ABOVE the spinal injury site (vasodilation)
- Bradycardia (heart rate less than 60 bpm)
- Pale, cool, clammy BELOW the spinal injury site (vasoconstriction)
- Goosebumps on the skin
- Sweating
- Dilated pupils/blurred vision
- Nasal stuffiness
- Anxiety
Nursing Interventions for Autonomic Dysreflexia
Think PDA
PREVENTION:
Think of the 3 BIG B’s (Bladder, Bowel, Break down of Skin)
Bladder: prevent distention by making sure the bladder stays emptied, assess urinary output, perform a bladder scans to make sure the bladder is not retaining urine (this is non-invasive), take steps to prevent urinary tract infections, if patient has a Foley catheter make sure it is draining properly (not kinked or blocked)
- If kinked, unkink it immediately.
- If clogged, may need to irrigate the Foley.
- If the patient is not catheterized and the bladder needs to be emptied, an anesthetic jelly (per MD order) should be used to prevent unnecessary irritating stimulation.
Bowel: assess last bowel movement, bowel sounds, and palpate abdomen for distention. If impacted, use an anesthetic jelly prior to manually removing the stool.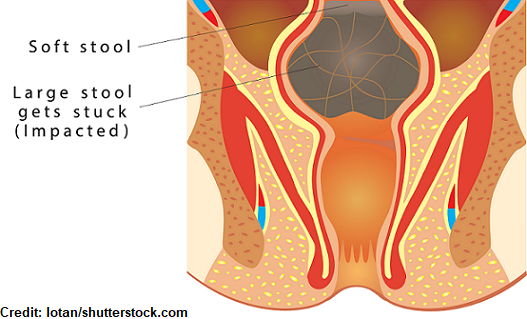
Break down of skin: remove any binding clothing or devices, turns every 2 hours, assess skin regularly, keep skin protected from injury etc.
DETECTION and ACTION:
Remember patients who’ve experience at T6 or higher spinal cord injury are at HIGHEST risk. Always assess blood pressure and monitor for any elevation (remember 20-40 mmHg higher from baseline could indicate AD).
- If patient reports a headache, INVESTIGATE it by checking blood pressure immediately.
- Monitor for the signs and symptoms above.
What to do if this develops: It’s a medical emergency!
- Get help (call rapid response), get help, and stay with the patient.
- Position the patient in High Fowler’s….90 degree angle with legs lowered….this will cause blood to pool in the lower extremities and help decrease blood pressure.
- Check blood pressure every 2-5 minutes.
- Remove any binding clothing or devices.
- Investigate and correct the problem….it could be any of the three Big B’s.
- Start with bladder (most common cause): assess that catheter is draining properly or if patient doesn’t have a Foley may need to be catheterize to drain urine (use anesthetic jelly to prevent more stimulation).
- Check for bowel impaction: need to use anesthetic jelly prior to prevent causing stimulation to the rectum and increase AD symptoms…remove stool if present.
- Check skin for injury or break down
If blood pressure still high may need medications:
- Nitropaste (topical application)….do NOT give Nitropaste if patient has taken a phosphodiesterase inhibitor within the past 24 hours (Sildenafil or Tadalafil) because this could lead to life-threatening hypotension.
- Nifedipine (sublingual for immediate release)…calcium channel blocker
References:
Allen KJ, Leslie SW. Autonomic Dysreflexia. [Updated 2019 Apr 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-.Available from: https://www.ncbi.nlm.nih.gov/books/NBK482434/
The Peripheral Nervous System | SEER Training. Retrieved from https://training.seer.cancer.gov/anatomy/nervous/organization/pns.html