This is an NCLEX review for pneumonia. Patients who have pneumonia are experiencing an infection of the lower respiratory system that affects the alveolar sacs. Pneumonia leads to impaired gas exchange which can require mechanical ventilation if severe enough.
In the previous review, I covered other respiratory disorders of the respiratory system. So, if you are studying for NCLEX or your nursing lecture exams be sure to check out that section.
When taking care of a patient who is experiencing pneumonia it is very important the nurse knows how to recognize the typical signs and symptoms seen in this condition, how it is diagnosed, nursing interventions, and patient education.
Don’t forget to take the pneumonia quiz.
In this NCLEX review for pneumonia, you will learn the following:
- Definition of Pneumonia
- Process of Gas Exchange
- Complication of Pneumonia
- Signs and Symptoms of Pneumonia
- Risk Factors of Pneumonia
- Types of Pneumonia
- How Pneumonia is Diagnosed
- Nursing Interventions for Pneumonia
- Antibiotics used to treat Pneumonia
NCLEX Lecture on Pneumonia Part 1 and Part 2
Pneumonia NCLEX Review Notes
Definition: a lower respiratory tract infection that causes inflammation of the alveoli sacs
Key Players:
- Germs: Bacteria, Virus, Fungi
- Lung Parenchyma: Alveoli, Alveolar Ducts, and Bronchioles (the trio in gas exchange)
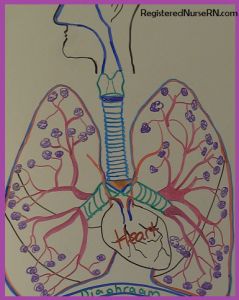 Process of normal gas exchange: oxygen is inhaled through the upper respiratory system down through trachea, the bronchus (right and left primary bronchi) which splits at the carina and enters into the lungs at the hilum and branches into the
Process of normal gas exchange: oxygen is inhaled through the upper respiratory system down through trachea, the bronchus (right and left primary bronchi) which splits at the carina and enters into the lungs at the hilum and branches into the
- Secondary Bronchi (also called Lobar Bronchi)
- Tertiary Bronchi (also called Segmental Bronchi)
then into smaller branches called bronchioles to the alveolar ducts to the alveolar sacs which inflate and deflate to allow gas exchange.
During this process, there is the transfer of oxygen from inhalation into the bloodstream and transfer of carbon dioxide out of the blood through the lungs which is exhaled. This happens in the alveoli capillary wall. Then the fresh oxygenated blood is taken back to the heart through the pulmonary vein and is pumped through the heart to the body.
How does Pneumonia develop?
Normally, the respiratory system can “fight off” these type of germs by filtering the air taken in through the nose and airway BUT certain conditions can damage the body’s ability to do this and make the body more susceptible to developing PNA.
These risk factors include:
- Prior infection: flu or cold
- Weak immune system: Elderly, infants, HIV, autoimmune medications
- Immobile: strokes or any other condition that causes decrease mental awareness or restrict ability to move
- Lung problems: COPD, asthma, smokers
- Post-opt patient: not coughing deep breathing
Nurse Sarah’s Notes and Merch
Just released is “ABG Interpretation Notes, Mnemonics, and Workbook by Nurse Sarah“. These notes contain 64 pages of Nurse Sarah’s illustrated, fun notes with mnemonics, and worksheets that include over 90 ABG practice problems and 60 test review questions covering ABG concepts.
You can get an eBook version here or a physical copy of the book here.
These germs get into the lungs by inhalation, aspiration, or from the blood and attack the alveoli sacs. These sacs become very inflamed and fill with fluid, body’s immune defense cell RBCs and WBCs, and bacteria.
 This causes the sac to lose the ability to inflate and deflate which allows proper gas exchange. Therefore, the patient will start to experience HYPOXEMIA (low oxygen in the blood) because oxygen cannot transfer across capillary wall to attach to RBCs to supply the body with oxygen and the body keeps the CO2 (carbon dioxide) which leads to RESPIRATORY ACIDOSIS!
This causes the sac to lose the ability to inflate and deflate which allows proper gas exchange. Therefore, the patient will start to experience HYPOXEMIA (low oxygen in the blood) because oxygen cannot transfer across capillary wall to attach to RBCs to supply the body with oxygen and the body keeps the CO2 (carbon dioxide) which leads to RESPIRATORY ACIDOSIS!
Arterial Blood Gase Values due to Respiratory Acidosis:
- ABGs: PO2: <90 mmHg
- pH: lower 7.35 mmHg
- PCO2: higher than 45 mmHg
- **To compensate for this the Kidneys start to conserve bicarbonate (HCO3) to hopefully increase the blood’s pH back to normal…..so HCO3 becomes >26 mEq/L
Further look at the Germs that Cause Pneumonia:
- Bacteria: most common cause of pneumonia especially in community-acquired is caused by Streptococcus pneumoniae
- Atypical Bacteria: Mycoplasma pneumoniae that causes “walking pneumonia” which is a milder form of pneumonia that isn’t severe enough to require complete bed rest
- Virus: influenza, RSV most common causes of PNA in children
- Fungi: least common…most likely to affect people with severe suppressed immune system and typically is contracted from outside in nature from plants, animals etc.
Types of Pneumonia
- Community-acquired Pneumonia (most occurring): patient obtains the germs that causes the pneumonia OUTSIDE of the healthcare system hence in the community.
- Hospital-acquired Pneumonia: patients who are on mechanical ventilation at major risk…it is hard to treat because the bacteria tend to be resistant to antibiotics and more likely a bacteria cause. Criteria: patient must have developed 48-72 hours after admission
Diagnosed:
- Notice: abnormal lungs sound when auscultating with stethoscope may hear coarse crackles, rhonchi (type of wheezing) or bronchial breath sounds which should be noted only in the tracheal area and this represents lung consolidation.
- Chest x-ray, sputum culture
Signs & Symptoms of Pneumonia
Remember the word: PNEUMONIA
Productive cough, Pleuritic pain (chest pain that is caused by coughing, breathing etc.)
Neuro changes (especially ELDERLY patients…may not even have a fever but fatigue and increased respiratory rate)
Elevated labs: PCO2 >45 (retaining carbon dioxide because it can’t pass capillary of alveoli sac), increased WBC (represents infection…body is trying to fight infection off)
Unusual breath sounds: coarse crackles, rhonchi, or bronchial in the peripheral lung fields
Mild to high Fever (bacteria cause produces highest fever….. greater than 104’F)
Oxygen saturation decreased (want >90%) will need supplementary oxygen
Nausea and vomiting (won’t feel like eating)
Increase heart rate and respirations
Aching all over with joint pain, Activity intolerance with shortness of breath
Nursing Interventions for Pneumonia
Monitor respiratory system:
- Lung Sounds
- Respiratory rate/vital signs
- Oxygen Saturation >95%
- ABGS (if ordered)
- Sputum (collect for culture)
- Suction as needed
Encourage usage of incentive spirometer for deep breathing and encourage coughing and deep breathing
Encourage 2-3 L of fluid (unless on fluid restriction as with patients who have heart failure)…fever causes dehydration, lose water through breathing (300-400 mL), and patient is too sick to have the urge to drink
Education on prevention: Up-to-date Vaccinations (Pneumovax every 5 years for patients 65+ and 19-64 years old with risk factors and annual flu shot)
Education about stop smoking, avoid people who are sick, hand-washing
Keeping head of bed elevated greater than 30 degree for immobile patients to prevent aspiration especially while eating and after meals along with frequent turning.
Breathing treatments and other respiratory therapy treatments (usually by respiratory therapy department). These will be schedule or PRN (as needed).
Treatments include: Bronchodilators, chest percussion etc.
Medications:
Administering per doctor’s order: fluids, antipyretics, antivirals (if a viral cause), and antibiotics (if a bacterial cause)
Antibiotics Groups for BACTERIAL Pneumonia
Remember the mnemonic: Various Medications Frequently Treat Pneumonia Cases
Antibiotics used depend on the bacteria type that is causing the infection, the patient’s ability to tolerate etc.
Vancomycin: used to treat severe cases and is one of the few that can treat bacteria that may be resistant to other antibiotics….watch for HEARING LOSS “ototoxicity”
Macrolides: “Zithromax (Z-Pak)” used in patients with Penicillin allergy….narrow-spectrum targets mainly gram positive bacteria
Tetracylines: “Doxycycline” broad-spectrum that targets gram positive and negative bacteria. Side effects: not for pregnant women or 8 years or younger due to growth retardation and teeth discoloration, photosensitivity of the skin and decreases effectiveness of birth control, no antacids or milk product while taking this medication because it affects absorption.
Fluroquinolones: “Levaquin” broad-spectrum (targets gram-negative and positive)…treatment for severe infection that are found in the hospital that are resistant. Side effects: c. diff infection, tendon rupture, cardiac arrhythmias such as QT interval prolonged
Cephalosporins: “Keflex, Rocephin” watch with patients who are allergic to penicillin (can also be allergic to cephalosporin)…great for community acquired pneumonia… ( 3rd and 4th generations of cephalosporins broad-spectrum)
Penicillin: “Penicillin G”…narrow-spectrum…target gram positive bacteria…. monitor if patient is allergic to cephalosporins, decreases effectiveness of birth control
Education about antibiotics: Take medications as prescribed and don’t stop in the middle of treatment….even if feeling better which helps decrease resistance
Viral Cases: May be prescribed an antiviral of the virus that is causing the pneumonia ex: Tamiflu
More NCLEX Reviews
References
- Help Prevent Pneumonia. Centers for Disease Control and Prevention. Retrieved 24 October 2016, from https://www.cdc.gov/pneumonia/
- Pneumonia – NHLBI, NIH. (2016). Nhlbi.nih.gov. Retrieved 25 October 2016, from https://www.nhlbi.nih.gov/health/health-topics/topics/pnu
- Treatment – NHLBI, NIH. Nhlbi.nih.gov. Retrieved 23 October 2016, from https://www.nhlbi.nih.gov/health/health-topics/topics/pnu/treatment