This NCLEX review will discuss cholecystitis.
As a nursing student, you must be familiar with cholecystitis and how to care for patients who are experiencing this condition.
These type of questions may be found on NCLEX and definitely on nursing lecture exams.
Don’t forget to take the cholecystitis quiz.
Lecture on Cholecystitis
Cholecystitis NCLEX Nursing Review
 Chole: bile
Chole: bile
Cyst: membranous sac
itis: inflammation
When you put all of this together you get: A membranous sac that contains bile is inflamed. Therefore, cholecystitis is the inflammation of the gallbladder.
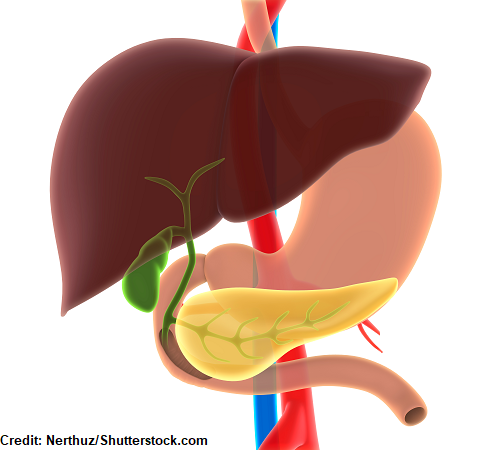
What’s the gallbladder?
It’s a dark green organ that is rotund in shaped. Some may say that it sort of looks like a little green pear.
The gallbladder is found under the liver on the right side of the body, which is very convenient since the liver and gallbladder are connected to each other and work together. They share their love for BILE!
Bile is greenish brownish substance and is created by the liver and travels to the gallbladder to be stored and concentrated via the hepatic ducts, which is why the organ is greenish in color.
Bile helps us digest and absorb fats that we consume like fat soluble vitamins such as A, D, E, and K. So, if our gallbladder isn’t working (like from a blockage or inflammation) our body can’t have access to these fats and they will exit the body as greasy/fatty stools called “steatorrhea”.
In addition, bile is also a vehicle for helping the body rid itself of bilirubin, which is created from the breakdown of old/worn out red blood cells. Bilirubin is a brownish/orange/yellowish substance and helps give our stool its brown color. So, if the gallbladder isn’t releasing bile properly (which contains bilirubin) the stool will become a light color (like clay), the sclera of the eyes could turn orange/yellow along with the skin (jaundice), and the urine will turn dark in color. This is because the bilirubin has leaked into the skin and urine rather than exiting the body in the stool.
How the gallbladder deals with bile?
The gallbladder squirts bile into the duodenum (a part of the small intestines). This happens when chyme (a thick semi-pulpy liquid that contains gastric juices and half-way digested food created by the stomach) enters into the duodenum which stimulates the gallbladder to contract. When this occurs, bile travels down the cystic duct and into the common bile duct and then into the duodenum. Bile will then fulfill its role with helping digest fats and help the bilirubin leave the body via stool.
Unfortunately, this process will become messed up when the gallbladder becomes inflamed and the gallbladder won’t be able to drain bile properly. Instead the bile will become thick and this will increase wall pressure within the gallbladder and lead to inflammation.
The inflammation can become so severe it can cause inflammation of the liver (hepatitis), pancreas (pancreatitis), sepsis, or perforate.
Causes of Cholecystitis
 Obstruction of some type:
Obstruction of some type:
- Cholelithiasis “gallstones”: main cause
- Risk factors: woman, obese, older, family history, pregnant, Native American or Mexican American
- Or any other type of obstruction in the gallbladder where bile can’t flow out via the cystic duct
—What happens? Bile stays in the gallbladder and becomes thick. This increases pressure in the gallbladder and damages the wall of the gallbladder, which causes inflammation and swelling of the gallbladder. Furthermore, due to the swelling and inflammation, blood flow to the gallbladder can be compromised and lead to death of the organ.
Acalculous “without a gallstone issue”: This is where the gallbladder is NOT working properly and it doesn’t contract
- This tends to occur to high acuity patient (very sick patients who are hospitalized), after surgery or during a severe illness like sepsis, burns, or major trauma, and even when a patient has been on TPN for a long period of time (the gallbladder isn’t being stimulated).
—What happens? Bile becomes thick and the gallbladder is not contracting like it should (not being stimulated) and this leads to inflammation.
Signs and Symptoms of Cholecystitis
- Nausea/Vomiting
- Pain in abdomen (epigastric) that tends to radiate to the right shoulder pain, especially after consuming a greasy meal
- Positive Murphy’s Sign: lay patient in supine position and palpate under the ribs on the right side at the midclavicular line. Then have the patient breathe out and then take a deep breath in. While the patient is breathing in, palpate on this area under the ribs…if the patient stops breathing in during palpation it is considered a positive Murphy’s Sign.
- Fever
- Bloating
- Steatorrhea, jaundice, dark brown urine, light colored stools (chronic cholecystitis)
Diagnosed? abdominal ultrasound, HIDA scan, or CT scan
Nursing Interventions for Cholecystitis
“Gallbladder”
GI rest
- NPO until recovered then clear liquids and advanced as tolerated per MD order
- When diet is ordered to be advanced assess how patient is tolerating the advancement…are they having nausea/vomiting, pain?
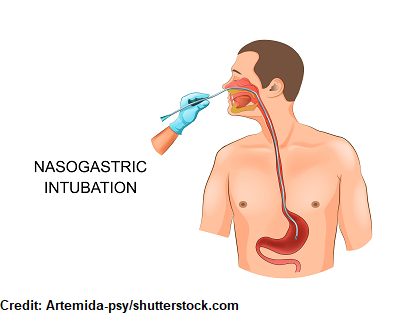
- Nausea/vomiting may be very severe and a nasogastric tube with GI decompression may be inserted. The NG tube, per MD order, may be set to low intermittent suction to help remove stomach contents so the gallbladder isn’t stimulated.
- Provide mouth care
- Provide mouth care
Analgesics for pain, antiemetics for nausea
Low-fat, gas-free foods diet when recovered
Large bore IV for fluids to hydrate and maintain electrolytes (many patients become dehydrated and have electrolyte imbalances from nausea and vomiting)
Breathing in stopped by patient during palpation of gallbladder because it hurts “Murphy’s Sign”
Labs: electrolytes, bilirubin (jaundice?), WBC, liver enzymes, pancreatic enzymes, renal function
Antibiotics for infection (IV)
Drain care
- Cholecystostomy tube “C-tube”: this is different than a t-tube which is sometimes placed after the removal of the gallbladder and is placed in the bile duct.
- C-tubes are place through the abdominal wall and into the gallbladder. They are for patients who can’t have surgery immediately to remove the gallbladder but the infected bile needs to be removed.
- It will drain infected fluid from the gallbladder.
- Things to remember:
- keep the collection bag at waist level to drain
- empty and record drainage
- Note color
- Monitor insertion site for infection
- Flush per MD order so it won’t get blocked and teach patient how to care for drain.
Deterioration signs and symptoms? How to tell if treatment is not helping and the patient is getting worst?
- Mental status changes, increased heart rate, decreased blood pressure, high temperature, high WBC, change in stool consistency and color (steatorrhea, light colored, jaundice, dark urine…no bilirubin), increasing or worsening abdominal pain (RUQ)
ERCP to remove the gallstones from the bile duct and assess areas of the gallbladder…an endoscope is inserted through the mouth and into the stomach to the small intestine and to the bile duct.
Removal of gallbladder “cholecystectomy”
- Since the gallbladder is removed bile will now drain from the liver via the bile duct into the duodenum.
- This procedure can be performed laparoscopically (most common) or open.
- Monitor for infection.
- Be aware that many patient who have the gallbladder removed laparoscopically will have shoulder pain from carbon dioxide (that was used during the procedure) not being reabsorbed by the body.
- Side lying with knees bent can help the pain along with heat application to the shoulders, or analgesics.
- Make sure the patient is ambulating soon after the procedure to prevent post-opt complications and coughing and deep breathing (splinting incision)…remind the patient how to use the incentive spirometer.
- T-Tube care:
- A t-tube works as a drain and it can be used for testing where dye is injected into the tube and an x-ray is taken to see if there are any more stones. It will light up the biliary tree.
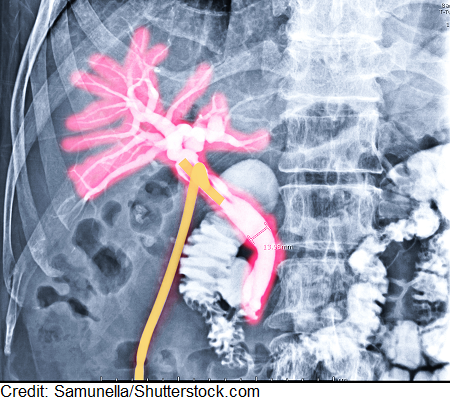
- The T part of the t-tube is placed in the bile duct to drain bile while the duct is healing after surgery because there will be swelling in the duct. It helps drain the excessive bile so it doesn’t all go into the small intestine because it will have to get use to having this amount of bile draining down (remember normally the gallbladder contracted and delivered it at intervals).
- Things to Remember:
- Patient will have a drainage bag that will need to be kept at the abdomen so it can drain properly and the patient should be upright in the Semi-Fowlers position to help with draining.
- Monitor drainage and that is it actually draining because it can become blocked.
- Drainage should NOT be more than 500 mL/day….first day post-op the drainage may be bloody and then will turn greenish/brown.
- Maintain skin care because bile is harsh on the skin.
- You must have a physician’s order to flush the t-tube.
- You may be ordered to clamped the tube 1 hour before and 1 hour after meals (MUST HAVE MD ORDER FOR THIS) so bile can enter the small intestine to help digest fats.
- When the tube is clamped monitor how the patient tolerates it….notify MD if the patient has nausea/vomiting, pain etc.
- A t-tube works as a drain and it can be used for testing where dye is injected into the tube and an x-ray is taken to see if there are any more stones. It will light up the biliary tree.
References:
Acute cholecystitis: MedlinePlus Medical Encyclopedia. Retrieved 12 September 2019, from https://medlineplus.gov/ency/article/000264.htm
Endoscopic Retrograde Cholangiopancreatography (ERCP) | NIDDK. Retrieved 12 September 2019, from https://www.niddk.nih.gov/health-information/diagnostic-tests/endoscopic-retrograde-cholangiopancreatography