This NCLEX review will discuss rheumatoid arthritis.
As a nursing student, you must be familiar with rheumatoid arthritis along with how to care for patients who are experiencing this condition.
These type of questions may be found on NCLEX and definitely on nursing lecture exams.
Don’t forget to take the rheumatoid arthritis quiz.
You will learn the following from this NCLEX review:
- Definition of rheumatoid arthritis
- Overview
- Signs and Symptoms
- Nursing Interventions
- Treatment
NCLEX Lecture on Rheumatoid Arthritis
Rheumatoid Arthritis NCLEX Review
What is rheumatoid arthritis? An autoimmune condition that causes inflammation in the joints. This inflammation specifically affects the membrane lining of the joint called the synovium. Rheumatoid arthritis can eventually lead to bone fusion.
What is a joint? It is where two bones meet together.
Rheumatoid Arthritis Stages:

Synovitis: inflammation of the synovium
WBCs invade the synovium, which causes it to become inflamed. This inflammation leads to thickening, and the formation of a pannus.
Formation of a Pannus:
A pannus is a layer of vascular fibrous tissue. The pannus will grow so large it will damage the bone and cartilage within the joint. The space in between the joints will disappear and anklyosis will develop.
Ankylosis:
This is the fusion of the bones. The patient will have major stiffness and immobility of the joint.
 Overview of Rheumatoid Arthritis
Overview of Rheumatoid Arthritis
The patient will have soft, tender, warm, and swollen joints. They will feel very tired (this leads them to be inactive) and have a fever.
**Hallmark signs: RA affects the same joint bilaterally. Stiffness and pain will be worst in the mornings (>30 minutes of stiffness) or after long periods of inactivity and all types of joints can be affected.
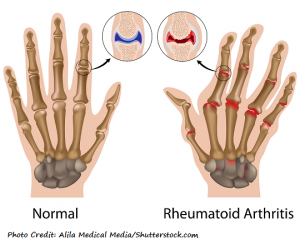
In the late stages bone deformity occurs (note the image below how the fingers are curved at the tops and it is symmetrical):

Rheumatoid arthritis most commonly affects the fingers and wrist. It can also affect the neck, shoulders, elbows, ankles, knee, and feet. However, it just doesn’t affect the joints but can extend to the heart, skin, eyes, mouth, lungs, and cause anemia.
Can happen at any age…most commonly 20-60 years old….not just in older adults as in osteoarthritis.
Cases vary: some patient have severe chronic cases that last for life time. While others may have for a short time and it goes into remission. RA can come on suddenly or gradually over years.
There is no cure for RA.
This key is to catch it early to prevent the progression of joint damage. Treatment includes:
- Medications: NSAIDs, corticosteroids, and DMARDs
- Surgery (replacing the joint with an artificial one, removal of the synovium “synovectomy”, “arthrodesis” (joint fusion) where the joint is removed and the bones are fused together with a bone graft.
It leads to the destruction of the joint within 2 years of the development of the disease, so it happens fast.
Management with:
- Lifestyle changes (developing plans for rest and exercise)
- Joint support: splints, using assistive device
- Stay healthy and low stress (cause flare-up)
Cause not clear (genetic, environmental, or hormonal factors)…tends to affect women more than men
Hard to diagnosis because symptoms may be associated with other diseases…tests typically ordered:
- Positive rheumatoid factor, elevated erythrocyte sedimentation, C-reactive protein (inflammation is present the body…higher in people with RA), x-ray shows joint deterioration
Signs and Symptoms of Rheumatoid Arthritis
Seven S’s
Sunrise Stiffness (severe pain)
Soft feeling in the joints
Swelling in the joint (warm)
Symmetrical
Synovium (affected and inflamed)
Systemic (affects not only the joints…patient will feel achy, tired, and it can affect the lungs, heart, anemia etc)
Stages (synovitis, pannus, anklyosis)
Nursing Interventions for Rheumatoid Arthritis
Nursing focus:
- Pain (need to know how to treat the pain)
- Preserving the joints (improving function and mobility, using assistive devices)
- Education (medications and nonpharmacological treatment, the disease itself)
- Mental status (dealing with depression and improving self-esteem, pain, alters life, no cure)
Joint assessment
Ask patient questions to help determine early on if this is RA: does it affect the symmetrical joints, when is the stiffness the worst?
Educate patient about the disease (no cure but can be managed) and assess patient’s understanding about RA because management (exercise, medications) help improve quality of life and prevent further joint deterioration.
Taking care of joints and decreasing fatigue:
During flare-ups rest the joints that are inflamed (no exercise on the joint)…splints help with this along heat and cold treatments:
- heat (best for stiffness)…heating pad or hot showers
- cold (best for pain….helps reduce inflammation)
Patient needs to maintain physical exercise as tolerated. This improves the fatigue and prevents a decrease in muscle strength. In addition, it prevents contractions by keeping the joints in motion.
Patient needs to schedule times for rest and to never overexert themselves.
Monitor for signs and symptoms of anemia (pale, fatigue, short of breath on excretion, palpations)….may be ordered supplements to promote RBCs production like iron, folic acid, vitamin b 12…at risk for GI bleeding due to medications NSAIDs….watch for dark, tarry stools
Multidisciplinary approach: Physical therapy and occupational therapy will be part of the patient’s care to help assist with treatment plans.
Patient needs to perform routinely ROM (range of motion) exercises and low impact aerobic exercise (stationary bike, walking, water aerobics)
Use assistive devices (make sure the patient is using them correctly to promote safety…at risk for injury). These devices help alleviate stress on the joints. These devices include raised toilet seat, tools to help grab items, tools to help button or zip shirts, shower chair, cane, walkers etc.
Medications for Rheumatoid Arthritis: combination of therapy may be used depending on the patient’s case
NSAIDs: decreases inflammation and helps with pain
- “Ibuprofen”: may cause GI distress…needs to be taken with food
Corticosteroids: decreases inflammation
- Dexamethasone (Decadron)
- Methylprednisolone (Medrol)
- Prednisone
- Can be given by mouth, topical, IV, injection into the joint or IM
- Skin become thins and fragile, bruises and tears easily….meticulous skin care
- Watch for hyperglycemia, especially in diabetic patients
- At risk for infection
DMARDs (disease-modifying antirheumatic drugs): suppresses immune system from attacking the joint along with helping slow down the destruction of the disease on the joints and bones.
- Hydroxychloroquine (Plaquenil) (monitor for vision changes…retinal damage)
- Leflunomide (arava)
- Methotrexate (Trexall)
- Sulfasalazine (Azulfidine)
DMARDS (biologic response modifiers): These drugs are still part of the DMARDs drug category but are genetically engineered and used in very severe cases.
- Abatacept
- Adalimumab
- No live vaccines, avoid infection (handwashing, avoid crowds and sick people), keeping appointments to measure blood levels (wbcs), injection site will be sore…common to have site reaction
More NCLEX Reviews
References:
- “Handout On Health: Rheumatoid Arthritis.” Niams.nih.gov. N.p., 2017. Web. 7 Aug. 2017.
- “Rheumatoid Arthritis (RA) | Arthritis Basics | Arthritis Types | Arthritis | CDC.” Cdc.gov. N.p., 2017. Web. 7 Aug. 2017.