This NCLEX review will discuss osteoporosis.
As a nursing student, you must be familiar with osteoporosis along with how to care for patients who are experiencing this condition.
These type of questions may be found on NCLEX and definitely on nursing lecture exams.
Don’t forget to take the osteoporosis quiz.
You will learn the following from this NCLEX review:
- Definition of osteoporosis
- Overview
- Signs and Symptoms
- Nursing Interventions
- Treatment
NCLEX Lecture on Osteoporosis
What is Osteoporosis? It’s a disease process that thins the bones to a point that the bones are not strong enough to withstand everyday stress and it breaks/fractures.
Most common type of fracture seen in patient with osteoporosis is called Colles’ fracture. This is a fracture of the lower part (distal) of the radius at the wrist.
What is happening to the bones in osteoporosis? The inside of the bone (specifically the spongy bone) becomes very porous and the bone’s density decreases….making it weak. Inside the spongy bone resides cells called osteoblasts and osteoclasts. Osteoclast CONSUME bone and osteoblasts BUILD bone. Normally, osteoblasts and osteoclasts work at the same rate. However, in osteoporosis the osteoclasts start to outwork the osteoblasts.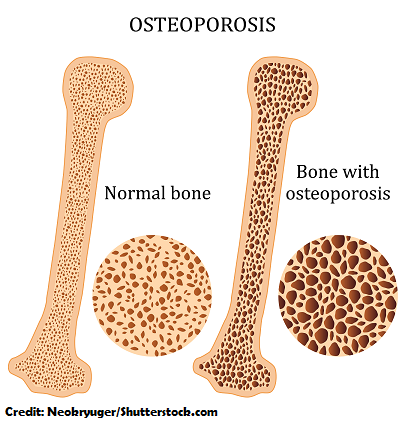 This disease suddenly sneaks up on a patient (in most cases without signs and symptoms). The patient is usually surprised with a bone fracture.
This disease suddenly sneaks up on a patient (in most cases without signs and symptoms). The patient is usually surprised with a bone fracture.
Osteoporosis most commonly affects the wrists, hips, and spine.
Role of the bones:
- Provides protection to our organs and supports them
- Allows us to move with the assistance of muscles, tendons, and ligaments
- Gives our body its shape
- Inside of the bones (specifically the bone marrow) there is an intricate system maintaining out survival:
- It’s responsible for red blood cell, platelet, and white blood cell production (red marrow)
- Storage of these blood cells along with storing our calcium and phosphorous minerals for when we need them
- Preserving lipids for energy when needed (yellow marrow)
Compact Bone vs. Spongy Bone
Compact Bone: is a strong, tight woven layer than protects the inside of the bone and helps maintain bone strength and resistance to stress
Spongy Bone: a matrix of pore-like components (hence its name “spongy”), such as proteins and minerals (calcium and phosphate). In osteoporosis this matrix starts to thin (it becomes more porous…making the bone weak).
- Within the spongy bone are OSTEOCLASTS (they consume the bone matrix and remove substances from the bone (calcium) and puts it in the bloodstream when we need it).
- OSTEOBLASTS (build up the bone matrix within the spongy bone by taking substances (phosphate and calcium) from the blood and building up the bone.
- These cells are majorly influenced by hormones (it is important to understand how these hormones work because this will help you understand the medication treatment which help slow down osteoclast activity):
Hormones that play a role in Bone Health:
Parathyroid hormone (PTH): When calcium levels are low the parathyroid gland secretes PTH (parathyroid hormone). This causes the osteoclasts to break down the stores of calcium in the bone so it can be placed in the blood….hence increasing calcium levels. In addition, PTH increases the small intestine reabsorption of calcium, and decreases the kidneys from excreting calcium.
- It is important to note that parathyroid hormone INDIRECTLY stimulates osteoclast activity. It plays a role with osteoblasts as well because PTH actually binds to osteoblasts.. In a sense the osteoblasts will control/regulate the activity of the osteoclasts under the influence of PTH. Therefore, if extra doses of PTH are given (as with the medication treatment drug Teriparatide “Forteo”) this can actually improve bone health by making the bone stronger and more resistant to fractures.
Calcitonin: When calcium levels are too high, the thyroid gland creates calcitonin to decrease the activity of the osteoclasts…..less break down of bones, which will keep calcium levels normal.
Growth hormone: stimulates osteoblasts to build up bones
Estrogen: controls the activity of osteoblasts and osteoclasts by keep the bones strong and prevent bone resorption by the osteoclasts. Estrogen in a nutshell prevents the osteoclasts from living too long.
- Why is this important to know? Remember estrogen is secreted by the ovaries. When a woman enters menopause she will produce less estrogen, which places her at risk for osteoporosis.
Testosterone: this is converted into estrogen to keep bones stronger, as stated above. As men age testosterone levels decrease and this puts them at risk for osteoporosis.
It is important to note that during a person’s mid 30’s most people reach peak bone mass. The osteoclasts and osteoblasts are working at the same rate. BUT after the mid 30’s the bones are broken down faster than replaced….hence why we see osteoporosis in older age.
Now let’s condense all the material above into a mnemonic to help us remember the risk factors:
Risk Factors for Osteoporosis:
Remember: “Calcium”
Calcium and vitamin D intake low (osteoclasts break down the bones more to keep calcium levels normal)
Age (bones become weaker as your age and bone mass decreases after 30, lower testosterone and estrogen levels)
Lifestyle (cigarette smoking, alcoholic, sedentary, immobile)
Caucasian and Asian women (women have less bone tissue than men)
Inherited (genetics)
Underweight BMI <19 (thin or small body frame..there is less bone mass and the person loses it quicker…anorexia)
Medications: glucocorticoids…three months or more (stimulates osteoclasts and decreases osteoblast activity), anticonvulsants: phenobarbital, carbamazepine (tegretol), phenytoin (Dilantin), valproate (Depakote) (affect the osteoclasts and osteoblast activity)
Signs and Symptoms of Osteoporosis:
“Frail”
Fracture (hip, wrist, spine) caused by normal regular activities
Rounding of the upper back Dowager’s Hump (spine deformity…stooped posture) from spine fracture
Asymptomatic until fracture
Inches of height lost overtime since a young adult (2-3 inches)…due to spinal fracture…can be painless
Low back pain, neck or hip pain (on palpation or with activity like bending or increase stress put on the bone)
Tests for Osteoporosis
Bone density test (BMD bone mineral density test): also called DXA or DEXA scan
- X-ray imaging taken to measure calcium and other bone minerals in the bones
- Patient Education: no calcium supplements (TUMS, ROLAIDS, other vitamins containing calcium etc.) 24 hours before the test
Nursing Interventions for Osteoporosis
Assessing for risk factors: remember the mnemonic CALCIUM
Discussing with patient how to change modifiable risk factors that can be changed
Assessing for possible signs and symptoms
Education about tests: DEXA scan: no calcium supplements 24 hours before test
Safety! Major concern…very simple fall can lead to a fracture…Patient needs the call light in reach at all times, room need to be clutter free, assistive devices (use correctly), non-slip sock, avoid rugs, watch pets getting around feet, using eyewear to see
Good body mechanics, ROM exercise
Prevention:
Weight-bearing exercise (helps increase bone mass)
- lifting weights, hiking, tennis…need stress of gravity on the bones to build them up…low-impact not as beneficial but good for cardiovascular health
Eating foods rich in calcium:
- Yogurt
- Sardines
- Cheese
- broccoli
- Collard greens
- Tofu
- Rhubarb
- Milk
Sufficient Vitamin D intake (helps body absorb calcium): salmon, tuna, cheese, egg yolks
Smoking cessation, limiting ETOH intake
Medications for Osteoporosis:
Calcium and Vitamin D supplements
Bisphosphonates: slows bone break down
- Alendronate (Fosamax), Risedronate (Actonel), Ibandronate (Bonvia)
- GI upset and esophagus problems: IMPORTANT!! Take with full glass of water in morning on empty stomach with NO other medications and sit up for 30 minutes or more…(60 minutes with Bonvia) after taking and don’t eat anything for 1 hour..helps the body absorb more of the medicine.
Calcitonin: made from salmon calcitonin, decreases osteoclast activity. Remember calcitonin is secreted by the thyroid gland naturally.
- At risk for HYPOcalcemia
Hormone replacement therapy (HRT) (estrogen): used for short-term due to other effects on the body: stroke, blood clots, breast cancer
Raloxifene (Evista): selective estrogen receptor modulator….monitor for deep vein thrombosis
Teriparatide (Forteo): severe cases of osteoporosis…it provides extra parathyroid hormone which stimulates osteoblasts and make them live longer
References:
- “Osteoporosis.” National Institute on Aging. N.p., 2017. Web. 5 Sept. 2017.
- “Osteoporosis Overview.” Niams.nih.gov. N.p., 2015. Web. 4 Sept. 2017.