This NCLEX review will discuss increased intracranial pressure (ICP).
As a nursing student, you must be familiar with this neuro disease along with how to provide care to a patient experiencing this condition.
Don’t forget to take the increased intracranial pressure quiz.
You will learn the following from this NCLEX review:
- Definition of increased ICP
- Pathophysiology
- Signs and Symptoms
- Nursing Interventions
- Medications
- Treatments
Increased Intracranial Pressure NCLEX Lecture
Increased Intracranial Pressure NCLEX Review
 What is increased intracranial pressure? It’s where pressure inside the skull has increased. This is a medical emergency!
What is increased intracranial pressure? It’s where pressure inside the skull has increased. This is a medical emergency!
Intracranial pressure is the pressure created by the cerebrospinal fluid and brain tissue/blood within the skull. It can be measured in the lateral ventricles.
What is a normal ICP: 5-15 mmHg (>20 mmHg…needs treatment)
Pathophysiology of Increased Intracranial Pressure
The skull is very hard and is limited on how much it can expand when something inside the skull experiences a change that leads to increased pressure.
Inside the skull are three structures that can alter intracranial pressure:
- brain
- cerebrospinal fluid (CSF)
- blood

To understand the patho of increased intracranial pressure, you must understand the Monro-Kellie hypothesis. It deals with how ICP is affected by CSF, brain’s blood, and tissue and how these structures work to maintain cerebral perfusion pressure (CPP).
In a nutshell, this hypothesis says that if the volume of one of these structures increases, the others must decrease their volume to help alleviate pressure. When there is an increase in intracranial pressure, the body can temporarily compensate for it by shifting CSF to other areas of the brain or spinal cord (or decrease it production), and alter blood volume going to the brain through vasocontriction, but if the pressure is continuous it is unable to compensate.
Intracranial pressure fluctuates and this can depend on many factors like:
- person’s body temperature
- oxygenation status, especially CO2 and O2 levels
- body position
- arterial and venous pressure
- anything that increase intra-abdominal or thoracic pressure (vomiting, bearing down etc.)
For the brain to receive proper nutrients to work it must receive a certain about of cerebral blood flow. This is the amount of blood flowing to the brain’s tissue. It does this by altering the cerebral perfusion pressure via vasoconstriction or vasodilation. For example, if carbon dioxide levels are abnormally high (>45) vasodilation occurs, which allows more blood volume to enter the brain. However, this is not good if a patient has increased ICP because this will further increase the ICP.
Cerebral perfusion pressure can become compromised during increased intracranial pressure. Therefore, there must be a sufficient cerebral perfusion pressure so that the brain is properly maintain.
What is a normal CPP? 60-100 mmHg
NOTE: When CPP falls too low the brain is not perfused and brain tissue dies. If the patient’s mean arterial pressure (MAP) starts to fall to the patient’s ICP, then the cerebral perfusion pressure will drop. Therefore, maintaining a sufficient MAP is essential.
So How is CPP calculated?
Equation: CPP= MAP – ICP
You need to know the following:
BP: 90/42
ICP: 19
First, the MAP must be calculated:
MAP= Diastolic BP x 2 + SBP divided by 3
42 x 2 = 84
84 + 90 = 174 ….divided by 3= 58 (MAP)
58-19= CPP 39….very low…normal 60-100 mmHg
What can cause an increased pressure within the skull that leads to increased intracranial pressure?
- injury (head trauma)
- increased in cerebrospinal fluid
- hemorrhage (hemorrhagic stroke…aneurysm bursts)
- hematoma (subdural and epidural…bleeding in between structures in the brain)
- hydrocephalus: buildup of CSF in the brain…normally flows through the brain and spinal cord and enters the bloodstream (blocked, too much is made)
- tumor: putting pressure on brain
- encephalitis (inflammation of brain tissue) or meningitis (inflammation of membrane covering spinal cord and brain)
What happens with increased intracranial pressure? Limited cerebral blood flow due to decreased cerebral perfusion from building pressure in the brain. The brain is getting squeezed and this leads to ischemia. All of this can lead to swelling and edema, which will eventually (if not treated) lead to herniation or displacement of the brain. The displacement of the brain can compress important areas of the brain like the brain stem (specifically medulla and vagus nerve).
When CPP falls too low the body tries to increase systolic blood pressure to make more blood go to the brain, but this makes things worst!! During this time the arteries will start to dilate because of the retention of carbon dioxide. This causes more blood to flow to the brain but this will compress veins and limit blood flow to the heart. Hence, leading to more swelling and even more ICP. As all this progresses the patient’s signs and symptoms will start to become worst. Therefore, it is essential to know the EARLIEST signs and symptoms (mental status changes) of increased ICP.
Signs and Symptoms of Increased ICP
“Mind Crushed”
Mental Status Changes ***Very earliest!! remember this for exam!! (restless, confused, problems performing normal movements and responding to questions)
Irregular breathing (slow down of respirations and irregular…cheyne-stokes…hyperventilation then apnea cyclic)*late
Nerve changes to optic and oculomotor nerve: double vision, swelling of optic nerve (papilledema), pupil changes (decreased, increased, or unequal size), abnormal doll’s eyes: oculocephalic reflex…in an unconscious patient open the eyes and move the head from side to side….if eyes don’t move in the opposite direction but stay fixed in a mid-line position this is a very bad sign….indicates brain stem damage
Decerebrate or decorticate posturing or flaccid
- Decorticate (flexor posturing): brings upper extremities to the core of the body (middle)
- adduction and flexion of arms, leg rotated internally, feet flexed

- Decerebrate: (Extension posturing): extends upper extremities from the body *worst of the two (remember all the E’s in decerebrate and think EXTEND arms)
- adduction and extension of arms with pronation, and feet flexed

Cushing’s Triad: LATE SIGN…herniation of the brain stem
- Increased systolic blood pressure (widening pulse pressure: increase in SBP and decrease in DBP), decreased heart rate, and abnormal breathing
- Increased SBP (due to body trying to get more blood to the brain…thinks it’s helping) ->
- Baroreceptor reflex (parasympathetic responds by dropping the heart rate to decrease the blood pressure and there may be compression of the vagus nerve due to compression from the swelling in the brain ->
- The compression on the medulla of the brain leads to abnormal respirations cheyne-stokes
Reflex positive Babinski (toe fan out…abnormal)
Unconscious LATE
Seizures
Headache
Emesis (vomiting) without nausea projectile
Deterioration of motor function (hemiplegia)…weakness on one side of the body
Nursing Interventions for Increased Intracranial Pressure
Focus on preventing further increase ICP and monitoring ICP (if monitoring device inserted)
“PRESSURE”
Position head of bed: 30 to 45 degree (helps blood return to heart), proper alignment of head (midline) NO flexion of neck (decreases venous return) or hips (increases intra-abdominal/thoracic pressure)…watching moving around in bed
Respiratory: Prevent HYPOXIA and HYPERCAPNIA! When blood oxygen levels drop or carbon dioxide levels increase, vasodilation occurs and this increases intracranial pressure.
- monitor blood gases, oxygen level, suctioning as needed only (no longer than 15 seconds…increase ICP) hyperoxygenated before and after
- mechanical ventilation to keep PaCO2 low 30-35 WHY? Vasoconstriction to help decrease ICP by decreasing blood flow….keep the PEEP low…increases intrathoracic pressure
Elevated temperature PREVENT this!
- Monitor temperature
- If patient is unconscious best to take tympanic, temporal or rectal route NOT orally or axillary….
- Why is there a risk for hyperthermia? Patient may have damage to the hypothalamus, infection, dehydration etc….a high temp. increases ICP, cerebral blood flow, and metabolic needs of the patient
- Can give antipyretics per MD order, remove extra blankets, decrease room temperature, cool baths…prevent shivering (increases metabolic needs and ICP)
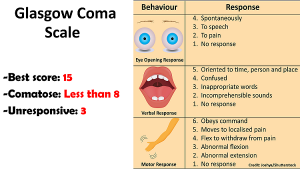
Systems to monitor: Glasgow Coma Scale
- neuro checks per protocol
- ventriculostomy (external ventricular drain): monitors ICP. It’s a catheter inserted in the area of the lateral ventricle to assess ICP and drains CSF during increased pressure readings.
- monitor for ICP levels greater than 20 mmHg and report to MD…..patients with increased ICP are not a candidate for lumbar puncture….risk of brain herniation.
Straining activities AVOIDED: vomiting, coughing, sneezing, Valsalva, agitation (keep environment calm), avoiding restraints as necessary
Unconscious patient care: avoid over sedating with narcotic or sedatives, lung sounds and suction as needed, immobile (skin breakdown, monitor nutrition, at risk for renal stones, constipation, passive range of motion with extremities) nutrition, eye care with solutions and ointments, maintain GI tubes for feeding (monitor residuals….poor gastric emptying more than 100 ml), blood clot formation (SCDs, passive range of motion), talk to the patient as you would a conscious patient
Rx: Barbiturates: to help decrease brain metabolism and BP which in turn decreases ICP, Vasopressors/IV fluids or antihypertensive to maintain SBP greater than 90 but less than 150, anticonvulsants meds, hyperosmotic drugs (leads to the next point of edema management)…….
Edema management: dehydrating the brain (must be done carefully…watching blood pressure and renal function)
Mannitol: it’s a concentrated type of sugar
When this drug enters the blood it is very concentrated and it draws water that is pooling in the brain back into the blood.
This type of diuretic is filtered through the glomerulus and not reabsorbed through the renal tubules, and because of this it creates an osmotic pressure that will pull water and electrolytes (sodium, chloride) from the blood (won’t be reabsorbed) and be excreted out.
Watch for fluid overload (water intoxication) and depletion.
FVO: signs and symptoms of heart failure, pulmonary edema (lung and heart sounds)
- monitor renal function, UOP, electrolytes
- not for patients with cerebral hemorrhage or anuria (no urine output)
- patient will report dry mouth and thirsty…provide mouth care
watch fluids (IV, oral), UOP, I and O’s (retention of urine?)
More edema management meds that may be ordered:
loop diuretics to remove fluid from brain and maintain a negative fluid balance….corticosteroids
References:
- Increased intracranial pressure, I. Increased intracranial pressure: MedlinePlus Medical Encyclopedia. Medlineplus.gov. Retrieved 7 January 2018, from https://medlineplus.gov/ency/article/000793.htm
- Intracranial pressure monitoring: MedlinePlus Medical Encyclopedia. Medlineplus.gov. Retrieved 8 January 2018, from https://medlineplus.gov/ency/article/003411.htm
- Traumatic Brain Injury: Hope Through Research | National Institute of Neurological Disorders and Stroke. Ninds.nih.gov. Retrieved 8 January 2018, from https://www.ninds.nih.gov/Disorders/Patient-Caregiver-Education/Hope-Through-Research/Traumatic-Brain-Injury-Hope-Through