This NCLEX review will discuss burns.
This review will include the types of burns, causes, nursing interventions, pathophysiology, and much more!
Don’t forget to take the FREE burns NCLEX quiz after reading this review.
Lecture on Burns
Burns NCLEX Review
What are burns? It is damage to the skin’s integrity from some type of energy source, such as:
- Heat (thermal): this can be hot liquid, steam, fire etc. that comes into contact with the skin…most common type
- Electrical: an electric current passes through the body and damages tissues
- It’s hard to determine the extent of damaged from this type of burn because the damage can extend under the skin. This is known as the “iceberg effect”.
- Watch for heart dysrhythmias and if the current is strong enough this can lead to bone fractures (watch for cervical spine injuries).
- Watch for renal failure: WHY? if the electrical current is strong enough this can cause the muscles to release myoglobin and cells to release hemoglobin. These substances block the tubules in the kidneys, which leads to acute tubular necrosis. This can happen with full-thickness burns as well because the muscle layer can be involved in this severe burn.
- Chemical: toxic substances come into contact with the skin (powders, gases, or certain foods…no heat needed). Remember alkali burns are harder to treat because these type of burns are NOT neutralized by the skin when compared to acidic burns.
- Cold: coldness comes into contact with the skin too long….example: frostbite
- Radiation: sun, treatments for cancer
- Friction: force abrasion to the skin….car accident…road rash, rope burn
Burn severity depends on:
- depth of damage to the skin
- percentage of the total surface of the skin affected (check out my video on rule of nines)
- patient’s age (children at most risk due to small size and elderly slower healing….usually have extensive medical history…skin is thin),
- medical history (diabetic already has issues with circulation already)
- where the burn is located (front and back of trunk, face and neck….THINK respiratory issues or is it a circumferential burn….a burn that “circles” or surrounds an extremity or the torso?
- did the patient experience an inhalation injury?
Therefore, if a patient has a large amount of total body surface area affected by a burn and the burns extends deep past the epidermis and dermis the patient is at risk for many problems…because severe burns affect all the systems of the body (immune system, renal, fluid/electrolytes, respiratory, GI etc. )
So, first let’s talk about:
Degrees of Burns (depth of burn damage)
There are first, second, third, and fourth degree burns….based on the depth of the burn… partial-thickness to full-thickness. However, to understand the various depth of burns let’s review the skin layers.
Skin Layers

Epidermis: top layer….it’s very thin compared to the dermis…keeps us protected for the environmental hazards…preventing infection.
Below that is the dermis, which is thicker than the epidermis….it contain the blood vessels along with the nerve endings, sweat/oil glands and the cells that help create new skin cells (thiswhy patients who have burns that involve deep into the dermis will need skin grafts because the body CAN’T remake the skin cells).
Below the dermis is the subcutaneous tissue (also called hypodermis): which contains fatty tissue, veins and arteries, nerves and helps insulate the muscles, bones, organs and REGULATES our body temperature. Patients who have burns that extend down into this layer will have problems regulating their body temperature.
Then below this are muscles, bones, and ligaments.
1st Degree (superficial): affects the top layer of the skin “epidermis”

- least severe of all the types
- heals usually within 7 days
- skin is very red or pink, painful, warm to touch, no blisters or usually no scar left behind
- brisk capillary refill (the faster the capillary refill, the more superficial the burn is)
2nd degree (partial-thickness) can be superficial or deep partial-thickness affecting various areas of the dermis

- involves the epidermis and dermis
- severity varies throughout…if severe (deep partial-thickness this burn can easily turn into 3rd degree)
- very painful…nerve sensation still present
- blister present
- redness that will blanch, swelling, shiny red/pink and moist in area
- may need skin grafting if severe
3rd degree: “full-thickness”: all skin layers are damaged along with the hair follicles, sweat glands, nerves

- not painful or the pain is dramatically decreased because damage to the sensation receptors
- skin can NOT heal…will need skin grafting
- months to heal
- can look black, yellow or red and hard and matte/dry
- can feel hard in areas or leathery….this is eschar which is hard, dead burnt tissue (will need to be removed for healing to occur and treatment)
- Eschar can be dangerous if it is present around the torso or an extremity….patient may need an escharotomy where the physician cuts the eschar to relieve pressure.
- How will you know an escharotomy was successful? The distal extremity has a pulse, is warm, and has a normal color. If on the torso, the patient will be breathing easier.
- Eschar can be dangerous if it is present around the torso or an extremity….patient may need an escharotomy where the physician cuts the eschar to relieve pressure.
4th degree “deep full-thickness” : worst of all…all the layers are destroyed but it extends to the muscles, bone, ligaments….all sensation of pain is gone.

- Appears black, charred with eschar
- >months to heal and needs skin grafting
********for full-thickness burns watch for ATN (acute tubular necrosis) because myoglobin and hemoglobin can be released into circulation…goes to kidneys and blocks perfusion, which leads to AKI (acute kidney injury).
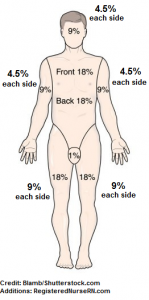
Rule of Nines for Burns in an Adult
 So what are the rule of nines?
So what are the rule of nines?
It’s a calculation used to calculate the total body surface area burned for burns partial-thickness or greater. The percentage will determine treatment like fluid replacement and if the patient meets the criteria for a burn unit.
The body is broken down in areas and nines are assigned to each area:
Start at the top and work downward (Remember THE FRONT AND THE BACK OF EACH AREA and there are two arm and two legs):
Adult:
Head and Neck: 9% (4.5% anterior and posterior)
Right Arm: 9% (4.5% anterior and posterior)
Left Arm: 9% (4.5% anterior and posterior)
Trunk: 36% (18% anterior and posterior)
Perineum: 1%
Right Leg: 18% (9% anterior and posterior)
Left Leg: 18% (9% anterior and posterior)
Practice problem:
A 35 year old female patient has deep partial thickness burns on the front and back of both arms, anterior trunk, back of left leg, anterior and posterior sides of the right leg, posterior head and neck, and perineum. What is the total body surface area percentage that is burned?
FRONT and BACK of both arms: 18%
ANTERIOR trunk: 18%
BACK of left leg: 9%
Anterior and Posterior of right leg: 18%
POSTERIOR head and neck: 4.5%
Perineum: 1%
Total: 68.5%
Another thing that determines burn severity is the location of the burn:
Exams like to ask about this and they will give you options about who is the most at risk with their burn injury. So, let’s talk about burn locations:
What areas on the body, if burned, will cause respiratory compromise?
- Face (this structure is where inhaling and exhaling starts and ends)
- Neck (contains structures that allow air to flow down into the lungs)
- Trunk (accessory muscles and structures to help you breathe) WHY? After severe burns there is a lot of swelling (edema) and if severe enough, tough leathery dead tissue called eschar can develop. This can impede respiratory movement, especially with circumferential type burns…plus the patient can have an inhalation injury and damage to the lung tissue.
What areas will have trouble healing because of poor blood supply (made of cartilage)? In addition to disfigurement, infection, and experience very slow healing?
- Ears and nose
What areas, if burned, will cause the most disability?
- Eyes, hands, feet, and joints
What areas are at most risk for infection?
- Areas used for elimination…..perineum and bottom
What type of burn and location is at risk for compartment syndrome?
Circumferential burns that are full-thickness (remember eschar is likely to develop). Location is the extremities……the circulation is being compromised to the distal extremity.
Next thing that determines burn severity is if the patient experienced an inhalation injury:
What is an inhalation injury? It’s damage to the respiratory system due to breathing in toxic substances associated with a burn: smoke, carbon monoxide, chemicals etc.
Why does breathing in carbon monoxide lead to death? The CO takes over on the red blood cell. Remember RBCs carry oxygen (with the help of hemoglobin found on the cell) throughout the body. Normally, RBCs have a very strong attraction to oxygen but when carbon monoxide molecules are present, the RBC prefers them over O2. This leads to no oxygen be transported throughout the body, which will eventually lead to death.
The upper and lower airways can be affected with an inhalation injury. The upper airway tends to be affected the most because the lower airway is usually protected by the glottis and vocal cord structures.
When would you suspect an inhalation injury in a patient? Remember these signs and symptoms!
- Burned in an enclosed structure
- Burn located on the face (especially mouth and nose)
- Carbonaceous sputum ….spit has soot in it…(smoke)
- Hair singeing on the head and nose hairs
- Soot in the mouth and nose (smoke)
- Skin bright red (CO poisoning)
- Trouble talking…voice is hoarse
- Confusion, anxiety
- Increased heart rate
Now let’s shift gears and talk about phases of burn management and the physiology of burns and mesh it will nursing interventions so you can easily understand the reason WHY you will be doing this specific nursing intervention.
Phases of Burn Management:
Remember “EAR”
Emergent: onset of the burn injury to restoration of capillary permeability (lasts 24-48 hours)
- Risk for: hypovolemic shock, respiratory distress, compartment syndrome
Acute: capillary permeability stabilized (diuresis) to wound close (starts 48-72 hours until wound heals)
- Focus: preventing infection, alieving pain, ensuring proper nutrition, wound care
Rehabilitative: burn healed to patient able to function again (mental and physical)
- Focus: psychosocial, ADLs, PT, OT, cosmetic correction
Physiology of Burns and Nursing Interventions for Burns
For this physiology discussion we are talking about a patient who has experienced partial to full-thickness severe burns on >15% or more on total body surface area. Simple burns don’t experience this type of physiological change in the body.
During the emergent phase, which is the first 24 hours, there is a huge change in the capillary permeability. This happens really fast….like 25 to 30 minutes fast! Remember our patient focus is fluid status!
What happens? Fluid (we’re talking about plasma) moves from the intravascular space into the interstitial tissue because the capillary bed is more permeable. Due to this SODIUM leaves with this plasma and this drops sodium levels in the blood….so you will see HYPOnatremia. In addition, albumin levels will drop because it leaves as well. What does albumin do? It regular oncotic pressure….in other words it regulates water…..so there will more spacing of fluid (swelling).
What will happen to the composition of the blood left in the intravascular space? Remember the fluid (plasma) that suspends the components of blood has left….so the blood will become very thick!! This will cause an INCREASE in the hematocrit level (it will actually decrease once fluids are replaced). The thickness of the blood will cause problems with micro-circulation. Cells are damaged from the injury: HYPERkalemia (damaged cell release potassium into the blood), WBC and immunoglobulins that help fight infection are damaged: AT RISK for INFECTION.
Problems for nurses to focus on: Fluid volume deficient (hypovolemic shock), electrolyte imbalances, potential renal failure and GI problems (due to fluid volume deficient, compartment syndrome (circumferential burns)
Hypovolemic shock: fluid left the intravascular system and there is a limited amount of fluid (hence blood) the heart can pump to the organs….will see an increased heart rate, decreased blood pressure, and decrease cardiac output
NEEDS FLUIDS!!!!
Fluid treatment is essential for major burns….the Parkland’s Burn Formula may be used to calculate the amount of fluids needed over the next 24 hours.
The formula calculates the amount of fluid (lactated ringers…LR) needed 24 hours after a burn (this is the time the patient received the burn….not arrived to you). It is used for patients who have partial-thickness (2nd degree burns) or higher.
Intravenous fluid resuscitation is needed for adults when a total body surface area of least 15% or more is burned for adults, and in 10% in children. (Diver, 2008)
To calculate the amount of LR needed 24 hours after a burn using the Parkland’s Burn Formula:….
Volume of Fluid needed (LR) = 4 mL x percentage of BSA x patient weight kilograms
How to give the fluids: 1/2 during the first 8 hours and then other 1/2 over the next 16 hours to equal 24 hours
Practice Problem:
A 46 year old male patient has partial thickness burns on:
- Anterior head and neck
- Front and back of left arm
- Front of right arm
- Posterior Trunk
- Front and back of right leg
- Back of left leg:
The patient weighs 180 lbs. Using the Parkland’s Burn Formula to calculate fluid replacement, calculate the hourly fluid rate (mL/hr) for this patient over the next 24 hours?
Answer: 1st 8 hours: 1,433 mL…..next 16 hours: 717 mL/hr
Rationale: 63% BSA burned
180 lb….divide by 2.2= 81.8….82 kg
4 mL x 63 x 82 = 20,664 mL of LR total
1st 8 hours: 22,932 divide by 2 = 11,466 mL…hourly rate (divide by 8): 1433.25…..1,433 mL/hr
Next 16 hours: 11,466 mL….hourly rate (divide by 16): 716.625……717 mL/hr
Nursing interventions: Monitor urinary output every hour!! UOP is the best way to determine if the patient is being hydrated properly. The patient will have a Foley catheter. You want to make sure the patient’s UOP is at least 30 cc/hr. If it is NOT contact the MD!
In addition, albumin may be ordered to help shift fluid back into the intravascular system.
What systems will experience changes due to the fluid shift?
Renal system: patient will be oliguric at first because of the shifting of blood, but then after about 24-72 hours diuresis will occur due to the stabilizing of the capillary system. Therefore, watch renal function and urinary output closely.
In addition, monitor the urine for hemoglobin and myoglobin if the patient has full-thickness or severe electrical burns…..acute tubular necrosis.
Gastrointestinal: there is decreased perfusion to the cells in the stomach that protect the stomach lining from the acid already in the stomach. These cells don’t work properly because of the decreased blood flow, and there is an increase in acid production because of the severe stress on the body. Therefore, the patient is at risk for CURLING’s ULCERS!!
In addition, the gut stops working and GI motility comes to a halt. In other words, an ileus can develop. This is where the GI system will not digest food.
Blood Glucose: levels can be increased because the stress response system causes the liver to release glycogen…..monitor glucose level.
Nursing Interventions: watch for reports of stomach pain (gnawing), vomiting, blood in stool)…..curling’s ulcer, administer antacids as prescribed, monitor bowels sounds (absent bowel sounds can indicate an ileus), nasogastric tube present to remove fluid, gas etc. Keep patient NPO until bowel sounds are present and you have an order to allow the patient to eat, maintain central line or feeding tube for nutrition
When GI function normal, the patient will need a high calorie, high protein and carb diet? WHY? Caloric intake is extremely high due to burn damage.
Circumferential burns are dangerous! Watch for compartment syndrome in the extremities:
- Distal extremity pulse is absent or weak, cool to the touch, abnormal color (white, blue, black), or has a sluggish capillary refill
- If located on the chest, watch respiratory status.
Respiratory system: monitor for inhalation injury, especially if on the face and neck……will need to be intubated
If carbon monoxide poisoning present: will need 100% oxygen with non-rebreather. Monitor carboxyhemoglobin levels…abnormal >15%
Infection: will need tetanus shot if not had one within the last 5 to 10 years
- Protective isolation: wear hair cover, shoe cover, gown, gloves, mask
- Use sterile linens and gowns
- Sterile gloves for dressing changes
- Strict hand hygiene
Temperature: lost the ability to regulate temperature….watch for shivering….room temperature 85-100’F.
Pain: IV best route WHY? Subq: skin layer damaged, IM: muscles can be damaged, GI (oral): remember the gut isn’t working like it should right now…..always select the option with IV route and PRE-MEDICATE before dressing changes or debridement procedures
Wound Care:
- Open dressing: open to air with topical antibiotic cream
- Closed dressing: topical antibiotic cream on burn and area covered with sterile dressing
- Debridement: necrotic tissue must be removed for healing to occur
- Cleaning wound via hydrotherapy or shower
- Positioning care with burns: NO pillows for the ear or neck (decreases blood flow and can lead to wound contractures)….use rolled towels under shoulders instead
- Elevate extremities and extend them to help prevent edema and prevent contractures.
- NEVER allow two burn areas to touch due to webbing that can occur.
- Range of motion and splints to prevent contractures.
References:
Burn Triage and Treatment – Thermal Injuries – CHEMM. Retrieved from https://chemm.nlm.nih.gov/burns.htm
Burn Triage and Treatment: Thermal Injuries – Radiation Emergency Medical Management. Retrieved from https://www.remm.nlm.gov/burns.htm
CDC – Carbon Monoxide Poisoning – Frequently Asked Questions. Retrieved from https://www.cdc.gov/co/faqs.htm
Diver, A. (2008). The evolution of burn fluid resuscitation. International Journal Of Surgery, 6(4), 347. Retrieved from https://www.sciencedirect.com/science/article/pii/S1743919108000290